

Clinical and biological predictors of response to standardised paediatric colitis therapy (PROTECT): a multicentre inception cohort study
- PMID: 30935734
- PMCID: PMC6501846
- DOI: 10.1016/S0140-6736(18)32592-3
Clinical and biological predictors of response to standardised paediatric colitis therapy (PROTECT): a multicentre inception cohort study
Abstract
Background: Lack of evidence-based outcomes data leads to uncertainty in developing treatment regimens in children who are newly diagnosed with ulcerative colitis. We hypothesised that pretreatment clinical, transcriptomic, and microbial factors predict disease course.
Methods: In this inception cohort study, we recruited paediatric patients aged 4-17 years with newly diagnosed ulcerative colitis from 29 centres in the USA and Canada. Patients initially received standardised mesalazine or corticosteroids, with pre-established criteria for escalation to immunomodulators (ie, thiopurines) or anti-tumor necrosis factor-α (TNFα) therapy. We used RNA sequencing to define rectal gene expression before treatment, and 16S sequencing to characterise rectal and faecal microbiota. The primary outcome was week 52 corticosteroid-free remission with no therapy beyond mesalazine. We assessed factors associated with the primary outcome using logistic regression models of the per-protocol population. This study is registered with ClinicalTrials.gov, number NCT01536535.
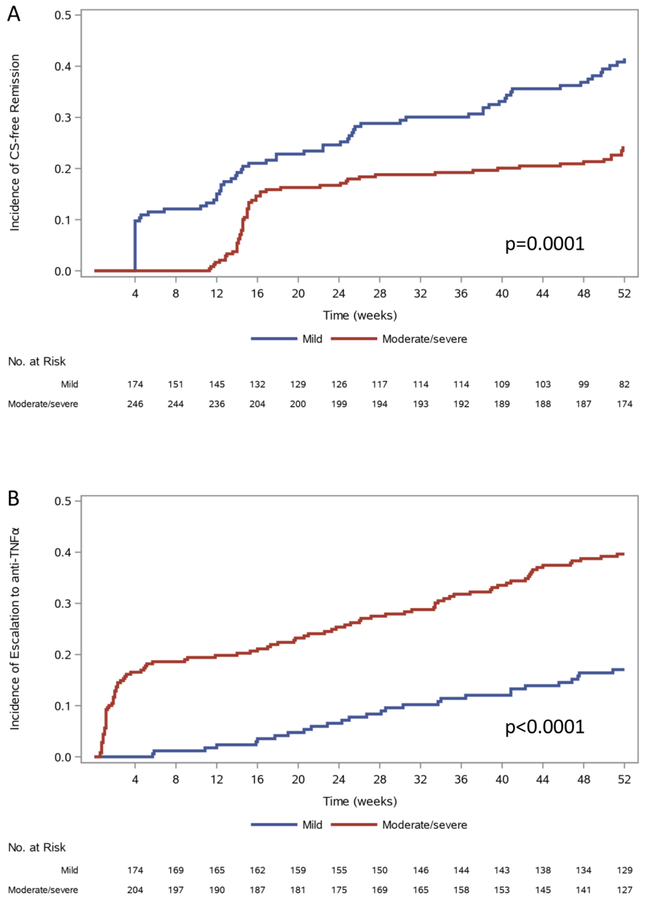
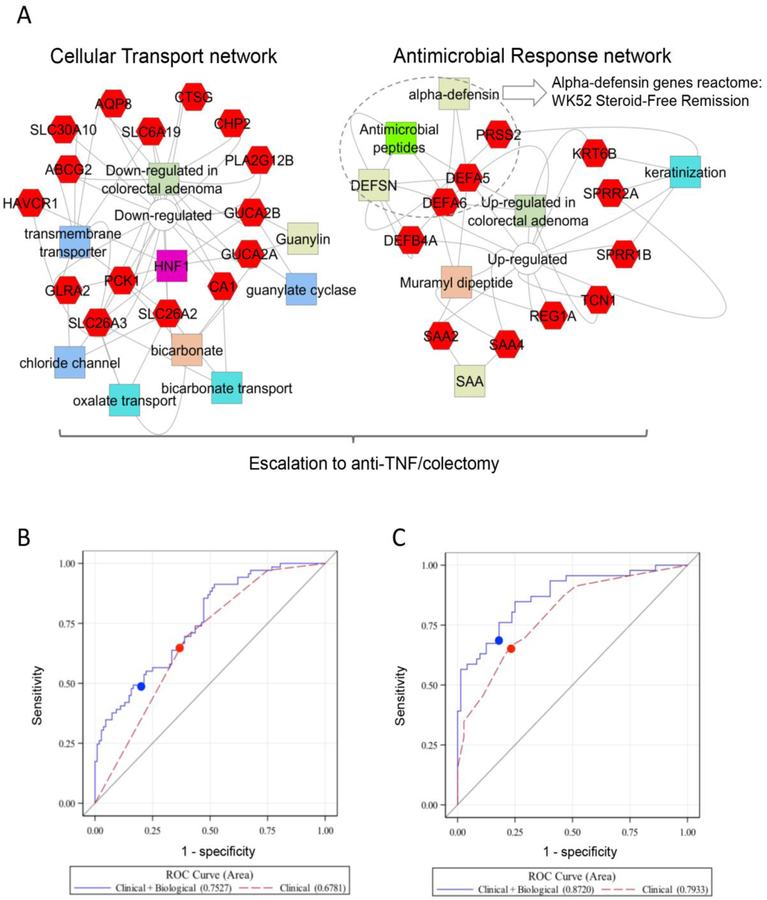
Findings: Between July 10, 2012, and April 21, 2015, of 467 patients recruited, 428 started medical therapy, of whom 400 (93%) were evaluable at 52 weeks and 386 (90%) completed the study period with no protocol violations. 150 (38%) of 400 participants achieved week 52 corticosteroid-free remission, of whom 147 (98%) were taking mesalazine and three (2%) were taking no medication. 74 (19%) of 400 were escalated to immunomodulators alone, 123 (31%) anti-TNFα therapy, and 25 (6%) colectomy. Low baseline clinical severity, high baseline haemoglobin, and week 4 clinical remission were associated with achieving week 52 corticosteroid-free remission (n=386, logistic model area under the curve [AUC] 0·70, 95% CI 0·65-0·75; specificity 77%, 95% CI 71-82). Baseline severity and remission by week 4 were validated in an independent cohort of 274 paediatric patients with newly diagnosed ulcerative colitis. After adjusting for clinical predictors, an antimicrobial peptide gene signature (odds ratio [OR] 0·57, 95% CI 0·39-0·81; p=0·002) and abundance of Ruminococcaceae (OR 1·43, 1·02-2·00; p=0·04), and Sutterella (OR 0·81, 0·65-1·00; p=0·05) were independently associated with week 52 corticosteroid-free remission.
Interpretation: Our findings support the utility of initial clinical activity and treatment response by 4 weeks to predict week 52 corticosteroid-free remission with mesalazine alone in children who are newly diagnosed with ulcerative colitis. The development of personalised clinical and biological signatures holds the promise of informing ulcerative colitis therapeutic decisions.
Funding: US National Institutes of Health.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Interests
These authors have nothing to disclose:
Alison Marquis, Nathan Gotman, Bradley Saul, Jessie Wang, David Mack, Francisco Sylvester, Jonathan Evans, Keith Benkov, Marian Pfefferkorn, Robert Baldassano, Susan Baker, Brendan Boyle, Stephen Guthery, Boris Sudel, Joshua Noe, Prateek Wali, Suresh Venkateswaran, Vin Tangpricha, Dedrick Moulton, Kevin Hommel, Jose Serrano, Krista Spada, Yael Haberman, Rebekah Karns, Melanie Schirmer, Ramnik Xavier, Angela Mo, Keith Benkov, Urko Marigorta, Greg Gibson
These authors report the following disclosures:
Jeffrey S. Hyams: Advisory Board, Janssen, Consultant, Abbvie, Takeda, Lilly, Boerhinger-Ingelheim, Allergan, Pfizer, Receptos, Astra Zeneca; Sonia Davis Thomas, independent data monitoring committee, Lycera Corporation; Lee A. Denson: Grant Support, Abbvie and Janssen,; Neal LeLeiko: Consultant, Abbvie; Ashish Patel, Speakers Bureau Abbvie, Janssen; James Markowitz,Consultant for Janssen, Celgene, Lilly; Maria Oliva-Hemker: Abbott Immunology—research grant, Janssen –research grant, Hoffman LaRoche—consultant; Anne Griffiths:: Research support Abbvie, Consultant Abbvie, Celgene, Janssen, Lilly, Pfizer, Takeda, Speaker Abbvie, Janssen, Shire; Joel Rosh:Consultant, Abbvie, Celgene, Janssen, Luitpold, Pfizer. Grant Funding Janssen, Abbvie; David Keljo: research support from Genentech and Takeda; Anthony Otley: Advisory Board, Janssen, Abbvie, Research support Lilly, Abbvie, Janssen, Takeda, Celgene; Michael Kappelman:Consultant, Abbvie, Janssen, GlaxoSmithKline, Pfizer; Marla Dubinsky: Consultant, Prometheus Laboratories, Abbvie, Janssen, Takeda, Pfizer, Celgene, UCB, Boehringer Ingelheim, Lilly, Gilead, Allergan; Paul Rufo: Consultant, Shire, Leutpold, Speaker, Abbvie, Research support, TechLab; Cary Sauer, Consultant, Abbvie; Margaret H. Collins, Consultant: Shire, Regeneron, Receptos, Allakos; Contracts with Shire, Regeneron; Subra Kugathasan, Consultant, Janssen, UCB; Jennifer Strople, Consultant and speaker, Abbvie; Melvin Heyman, Research grants Genentech, Abbvie, Shire, Takeda, Mallinkrodt, Janssen, Gilead, David Ziring, Speaker’s bureau: Abbvie, consultant 11th Health and Vitality Biopharma.
Figures
Comment in
-
Personalised therapy for inflammatory bowel disease.Lancet. 2019 Apr 27;393(10182):1672-1674. doi: 10.1016/S0140-6736(18)33125-8. Epub 2019 Mar 29. Lancet. 2019. PMID: 30935733 No abstract available.
References
-
- Gower-Rousseau C, Dauchet L, Vernier-Massouille G, et al. The natural history of pediatric ulcerative colitis: a population-based cohort study. Am J Gastroenterol 2009;104:2080–8. - PubMed
-
- Turner D, Mack D, Leleiko N, et al. Severe pediatric ulcerative colitis: a prospective multicenter study of outcomes and predictors of response. Gastroenterology 2010;138:2282–91. - PubMed
-
- Hyams JS, Davis P, Grancher K, Lerer T, Justinich CJ, Markowitz J. Clinical outcome of ulcerative colitis in children. J Pediatr 1996;129:81–8. - PubMed
-
- Melson JE, Giusto D, Kwasny M, Eichenseer P, Jakate S, Keshavarzian A. Histopathology predictors of medically refractory ulcerative colitis. Dis Colon Rectum 2010;53:1280–6. - PubMed
