

Does Tranexamic Acid Improve Clot Strength in Severely Injured Patients Who Have Elevated Fibrin Degradation Products and Low Fibrinolytic Activity, Measured by Thrombelastography?
- PMID: 30936005
- PMCID: PMC6874093
- DOI: 10.1016/j.jamcollsurg.2019.03.015
Does Tranexamic Acid Improve Clot Strength in Severely Injured Patients Who Have Elevated Fibrin Degradation Products and Low Fibrinolytic Activity, Measured by Thrombelastography?
Abstract
Background: Elevated d-dimers in injured patients with paradoxically low fibrinolysis activity measured by viscoelastic assays have been speculated to be "occult" fibrinolysis. However, an alternative explanation is that these patients have previously activated their fibrinolytic system and have shut it down by the time of blood draw, and would gain no benefit in clot strength with tranexamic acid (TXA). We hypothesize that TXA will not increase clot strength in injured patients with low fibrinolytic activity measured by thrombelastography (TEG), despite biomarkers of fibrinolysis activation.
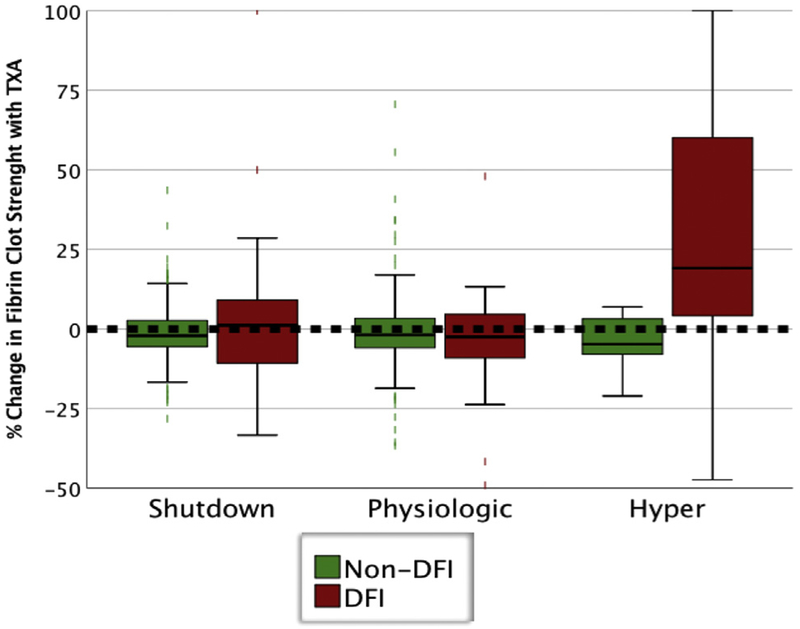
Study design: Three TEG assays (rapid, tissue plasminogen activator, and functional fibrinogen) were run on trauma patients. The tissue plasminogen activator TEG served as a functional assay to quantify depletion of fibrinolysis inhibitors (DFI). Patients were stratified by DFI vs non-DFI and then by rapid TEG lysis at 30 minutes phenotype cutoffs. Response to TXA was evaluated with functional fibrinogen TEG by calculating percent change in clot strength with the addition of exogenous TXA in the TEG cup.
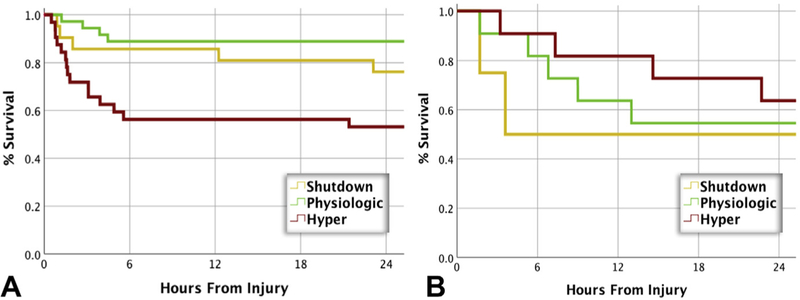
Results: Six hundred and thirty patients with a median new injury severity score of 20 were analyzed. Depletion of fibrinolysis inhibitors was present in 116 (18%). The DFI patients had significantly increased d-dimer (p < 0.001) and lower fibrinogen (p < 0.001). The DFI patients had increased rates of massive transfusion (33% vs 3.3%; p < 0.001) and mortality (40% vs 6.2%; p < 0.001). Among DFI patients, TXA significantly improved fibrin clot strength with hyperfibrinolysis (+19% clot strength; p < 0.001) but not with shutdown (+1.2%) or physiologic (-2.5%).
Conclusions: Patients with DFI have multiple abnormalities of their coagulation system, but only DFI patients with hyperfibrinolysis have improved fibrin clot strength with TXA.
Copyright © 2019. Published by Elsevier Inc.
Figures
Comment in
-
Discussion.J Am Coll Surg. 2019 Jul;229(1):101-103. doi: 10.1016/j.jamcollsurg.2019.05.012. J Am Coll Surg. 2019. PMID: 31248516 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
