

Review
doi: 10.2215/CJN.09630818.
Epub 2019 Apr 1.
Clinical Pharmacology in Diuretic Use
Affiliations
- PMID: 30936153
- PMCID: PMC6682831
- DOI: 10.2215/CJN.09630818
Item in Clipboard
Review
Clinical Pharmacology in Diuretic Use
Clin J Am Soc Nephrol.
.
Erratum in
-
Correction.Clin J Am Soc Nephrol. 2019 Nov 7;14(11):1653-1654. doi: 10.2215/CJN.09840819. Epub 2019 Sep 26. Clin J Am Soc Nephrol. 2019. PMID: 31558483 Free PMC article. No abstract available.
No abstract available
Keywords: Algorithms; Cardio-Renal Syndrome; Clinical; Distal; Diuresis; Edema; Gastrointestinal Absorption; Kidney Tubules; Metabolic Networks and Pathways; Pharmacology; Sodium Potassium Chloride; Symporter Inhibitors; diuretics; heart failure; nephrotic syndrome.
Figures
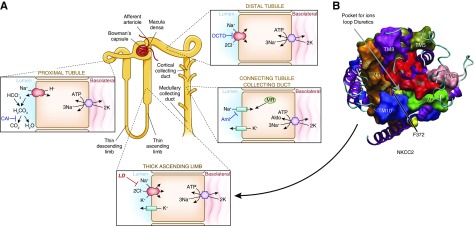
Sites of sodium reabsorption and diuretic action along the nephron. (A) Nephron figure showing percentages of sodium reabsorption by associated segment. (B) Homology structural model of the loop diuretic–sensitive NKCC2 viewed from the extracellular surface. The pocket for ion translocation and diuretic binding is shown by the arrow. Mutation of a key phenylalanine (F372) alters diuretic binding (reconstruction adapted from Somasekharan et al. [2]). Aldo, aldosterone; Aml, amiloride (and triamterene); CAI, carbonic anhydrase inhibitors; DCTD, distal convoluted tubule diuretic; LD, loop diuretics; MR, mineralocorticoid receptor, site of spironolactone and eplerenone action (not shown).
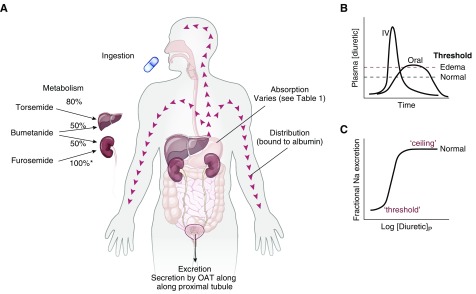
(A) Features of absorption, distribution, metabolism, and excretion (so-called ADME) of drugs. (B) Comparing the plasma diuretic concentration as a function of time after oral or intravenous diuretic administration. The dashed lines show natriuretic thresholds in normal individuals and in those with edema. Note that the primary determinant of natriuresis is the time above the threshold, indicating why route of administration has different effects in stable patients and in those with severe edema. In a normal individual, an oral dose may be effective, whereas it may not be in edema despite retained bioavailability. (C) Classic dose-response curve, plotted versus the logarithm of the plasma concentration. Note the threshold for natriuresis and the maximal level, often called the ceiling. IV, intravenous.
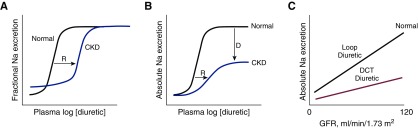
Pharmacokinetics and pharmacodynamics of diuretic action. (A) Effects of CKD on diuretic actions. Note that in CKD, baseline fractional sodium excretion is high, to maintain absolute rates of sodium excretion equal to intake. There is a shift in the dose-response curve to the right (R), primarily owing to impaired diuretic secretion, but no change in the ceiling effect. (B) The same relationship plotted versus absolute rates of sodium excretion. The same rightward shift is evident, but the ceiling is lower, owing to the GFR reduction (as indicated by D). (C) Comparing effects of loop diuretics and distal convoluted tubule (DCT) diuretics on absolute sodium excretion, given a retained effect on fractional excretion.
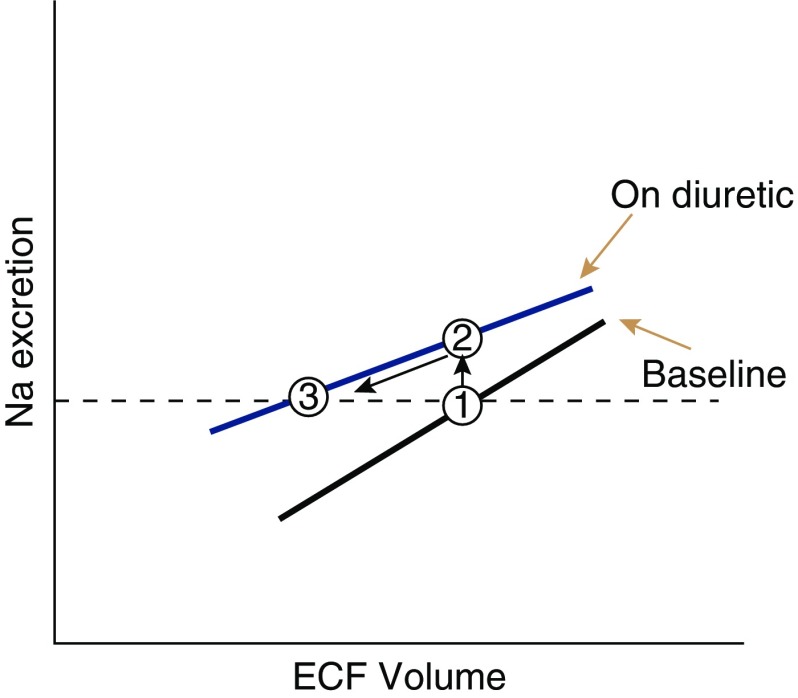
Relationship between ECF volume and sodium excretion, based on (57). Diuretics shift this curve upward (blue line), but may make it shallower. The baseline sodium excretion rate (which equals intake) is shown by the dashed line. After a diuretic is started, urinary sodium excretion rises by shifting to a new curve (from point 1 to point 2). Gradually (through the braking phenomenon) urinary sodium excretion declines back to the baseline level, but at a new and reduced ECF volume (from point 2 to point 3).
References
-
- Hammarlund MM, Paalzow LK, Odlind B: Pharmacokinetics of furosemide in man after intravenous and oral administration. Application of moment analysis. Eur J Clin Pharmacol 26: 197–207, 1984 - PubMed
-
- Brater DC, Day B, Burdette A, Anderson S: Bumetanide and furosemide in heart failure. Kidney Int 26: 183–189, 1984 - PubMed
-
- Shankar SS, Brater DC: Loop diuretics: From the Na-K-2Cl transporter to clinical use. Am J Physiol Renal Physiol 284: F11–F21, 2003 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
