

Risk of severe maternal morbidity associated with cesarean delivery and the role of maternal age: a population-based propensity score analysis
- PMID: 30936165
- PMCID: PMC6443524
- DOI: 10.1503/cmaj.181067
Risk of severe maternal morbidity associated with cesarean delivery and the role of maternal age: a population-based propensity score analysis
Abstract
Background: Short-term maternal complications of cesarean delivery remain uncertain because of confounding by indication. Our objective was to assess whether cesarean delivery is associated with severe acute intra- or postpartum maternal morbidity compared with vaginal delivery, overall and according to the timing of the cesarean.
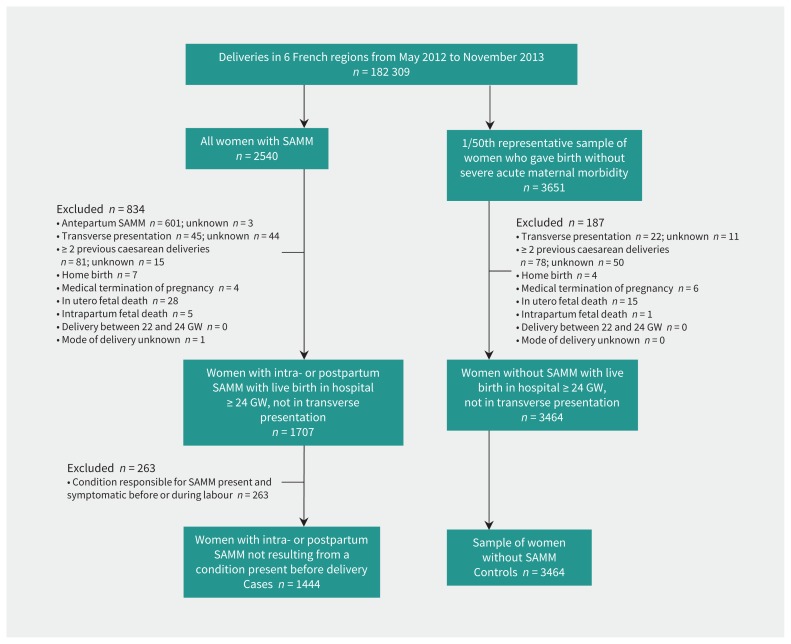
Methods: We performed a case-control analysis using data from EPIMOMS, a prospective population-based study of deliveries at 22 gestation weeks or later from 6 regions of France in 2012-2013. Cases of intra- or postpartum severe acute maternal morbidity that were not a result of a condition present before delivery were compared with controls randomly selected in a 1/50 ratio. Associations between delivery modes and severe acute maternal morbidity were estimated in a propensity score-matched sample.
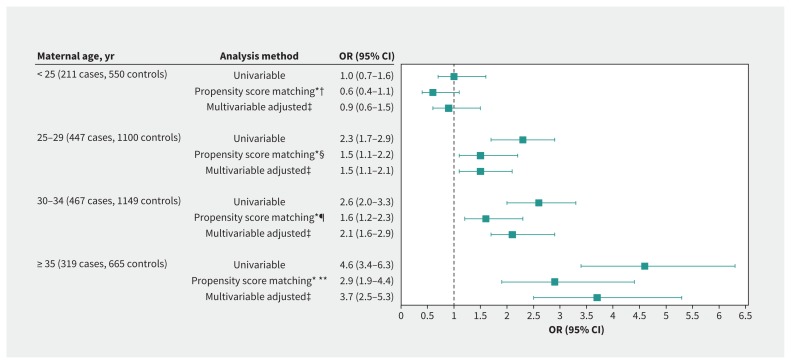
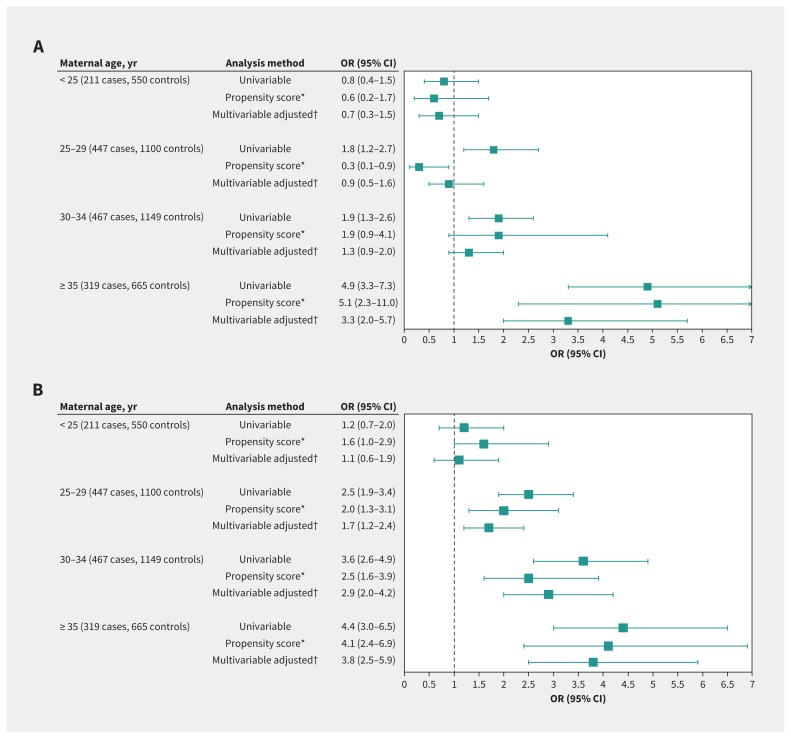
Results: Among 182 300 deliveries, we identified 1444 cases and 3464 controls. The proportion of cesarean delivery was significantly higher among cases than controls (36.0% v. 18.2%). In the propensity score-matched analysis, cesarean deliveries were significantly associated with a higher risk of severe acute maternal morbidity (adjusted odds ratio [OR] 1.8, 95% confidence interval [CI] 1.5-2.2). This association increased with maternal age and was particularly marked for women aged 35 years or older (adjusted OR 2.9, 95% CI 1.9-4.4). This increased risk was significant for cesarean deliveries during labour in women of all age groups and for those before labour only in women aged 35 years or older (adjusted OR 5.1, 95% CI 2.3-11.0).
Interpretation: Cesarean delivery is associated with a higher risk of severe acute maternal morbidity than vaginal delivery, particularly in women aged 35 years and older. Clinical decisions regarding delivery mode should account for this excess risk accordingly.
© 2019 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Delivery options and risk of severe acute maternal morbidity.CMAJ. 2019 Aug 19;191(33):E922. doi: 10.1503/cmaj.72609. CMAJ. 2019. PMID: 31427359 Free PMC article. No abstract available.
-
Key considerations when comparing outcomes by mode of delivery raise questions about study validity and clinical relevance.CMAJ. 2019 Aug 19;191(33):E923. doi: 10.1503/cmaj.72687. CMAJ. 2019. PMID: 31427360 Free PMC article. No abstract available.
References
-
- The European Perinatal Health Report: health and care of pregnant women and babies in Europe in 2010. Euro-Peristat; 2013. Available: www.europeristat.com/Reports/European-Perinatal-Health-Report-2010.Html (accessed 2018 Aug. 10).
-
- Scott JR. Cesarean delivery on request: Where do we go from here? Obstet Gynecol 2006;107:1222–3. - PubMed
-
- Meikle SF, Steiner CA, Zhang J, et al. A national estimate of the elective primary cesarean delivery rate. Obstet Gynecol 2005;105:751–6. - PubMed
-
- Parrish KM, Holt VL, Easterling TR, et al. Effect of changes in maternal age, parity, and birth weight distribution on primary cesarean delivery rates. JAMA 1994;271:443–7. - PubMed