

State of care for patients with systemic autoinflammatory diseases - Results of a tertiary care survey
- PMID: 30937142
- PMCID: PMC6439415
- DOI: 10.1016/j.waojou.2019.100019
State of care for patients with systemic autoinflammatory diseases - Results of a tertiary care survey
Abstract
Background: Systemic autoinflammatory diseases (SAIDs) are rare debilitating disorders of which there is limited awareness and a significant delay in diagnosis. There is no uniform approach in the diagnosis and treatment of these disorders and the real life state of SAID patient care is poorly characterized. The aim of this study was to obtain data on the epidemiology, state of care and the perception of physicians who are involved in the care of SAID patients.
Methods: We performed a questionnaire-based survey and contacted 134 university departments of dermatology, pediatrics, rheumatology and other SAID departments of tertiary care in German-speaking countries.
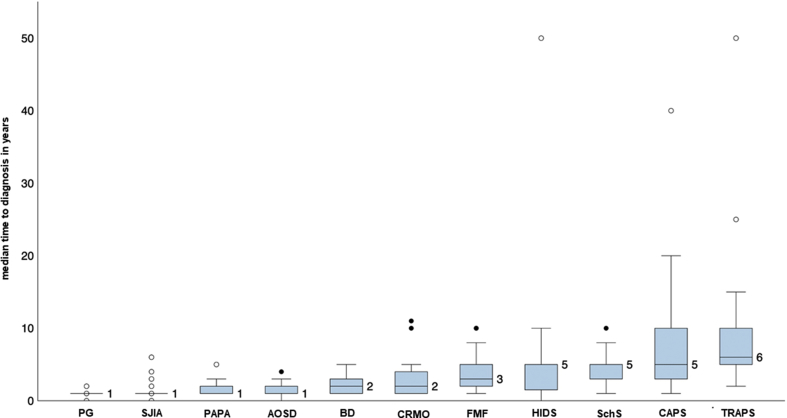
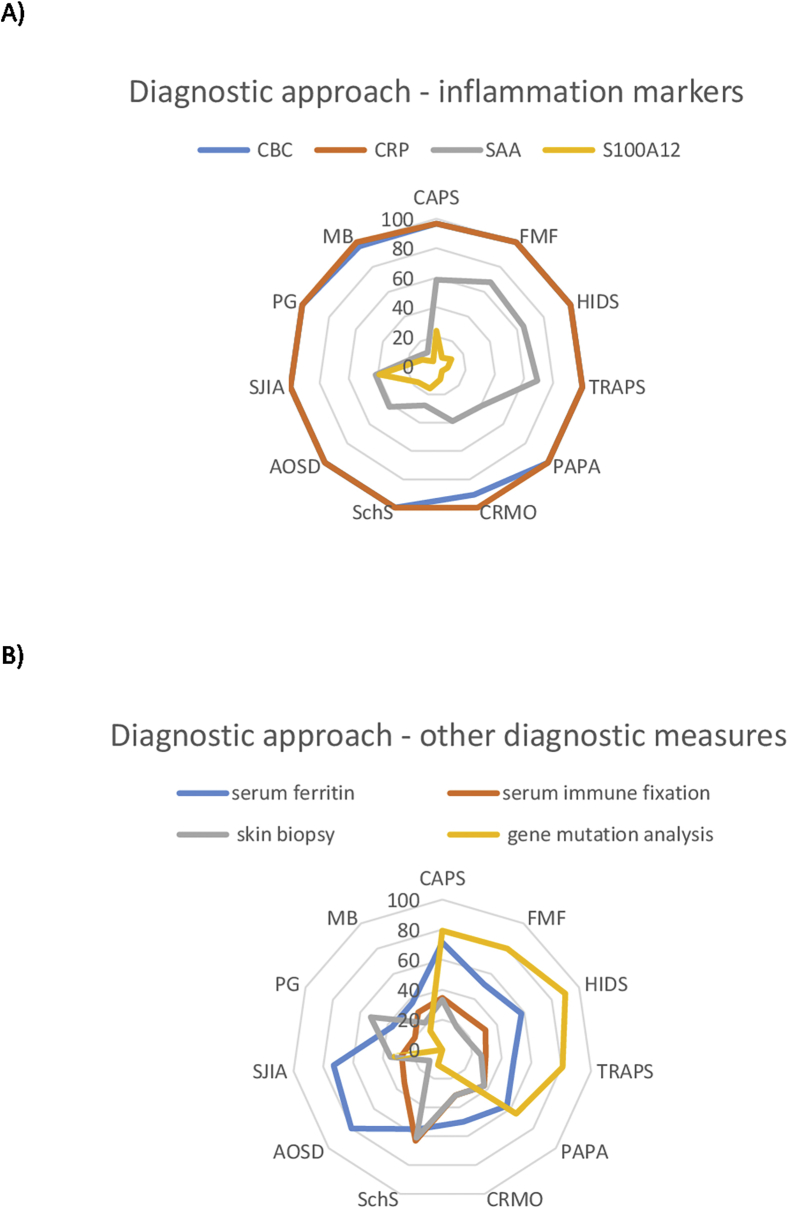
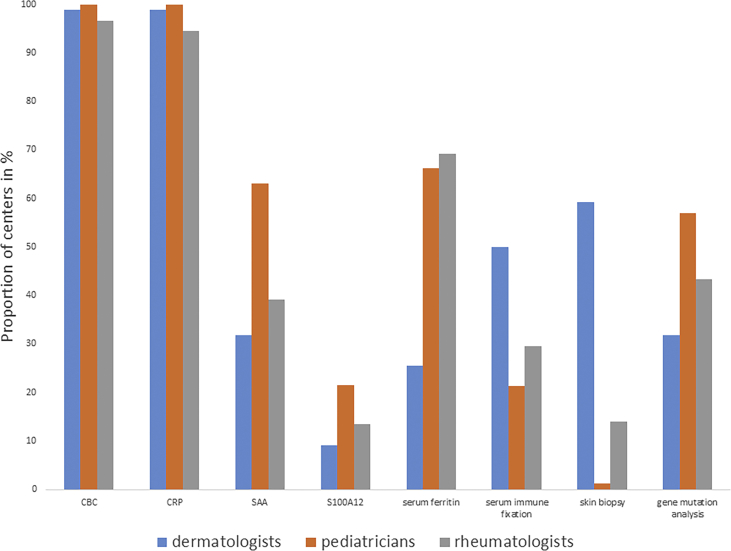
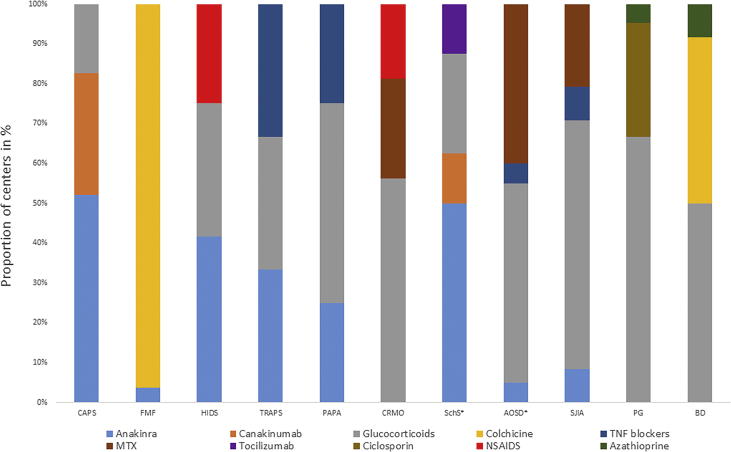
Results: A total of 37 departments participated in the survey. The majority of departments managed both adult and pediatric patients with a variety of monogenic and polygenic/acquired SAIDs. For monogenic SAIDs such as cryopyrin-associated periodic syndromes (CAPS) and familial Mediterranean fever (FMF), the diagnostic and treatment strategies were similar among the departments. The diagnostic work-up included inflammatory markers and genetic testing, the first line treatment interleukin-1 (IL-1) blockers for CAPS and colchicine for FMF. For polygenic/acquired SAIDs, we observed a significant heterogeneity in diagnostic and therapeutic approaches. As a major unmet need, diagnostic delay was identified with a median time to diagnosis of 2 (range 1-5) years. The overall state of care for SAID patients was rated to be excellent or good by only 12% of departments, and to be poor or non-sufficient by 40% of departments.
Conclusion: This study demonstrates a high need to improve the state of care and to harmonize diagnostic and treatment strategies for SAID patients.
Keywords: AOSD, Adult-onset Still's disease; ARC2, Autoinflammation Reference Center Charité; Autoinflammatory disease; BD, Behçet's disease; CAPS, Cryopyrin-associated periodic syndrome; CBC, Complete blood count; CRMO, Chronic recurrent osteomyelitis; CRP, C-reactive protein; FMF, Familial Mediterranean fever; HIDS, Hyper IgD syndrome; IL-1β, Interleukin-1β; MKD, Mevalonate kinase deficiency; MWS, Muckle-Wells syndrome; NSAIDs, Nonsteroidal anti-inflammatory drugs; PAPA, Pyogenic arthritis pyoderma gangrenosum and acne syndrome; PG, Pyoderma gangrenosum; PRAAS, Proteasome-associated autoinflammatory syndrome; SAA, Serum amyloid A; SAIDs, Systemic autoinflammatory diseases; SJIA, Systemic juvenile idiopathic arthritis; SchS, Schnitzler's syndrome; State of care; Survey; TNF, Tumor necrosis factor; TRAPS, TNF-receptor-associated periodic syndrome.
Figures
References
-
- Grateau G., Hentgen V., Stojanovic K.S., Jeru I., Amselem S., Steichen O. How should we approach classification of autoinflammatory diseases? Nat Rev Rheumatol. 2013;9(10):624–629. - PubMed
-
- Kuemmerle-Deschner J.B., Ozen S., Tyrrell P.N. Diagnostic criteria for cryopyrin-associated periodic syndrome (CAPS) Ann Rheum Dis. 2017;76(6):942–947. - PubMed
-
- Gusdorf L., Asli B., Barbarot S. Schnitzler syndrome: validation and applicability of diagnostic criteria in real-life patients. Allergy. 2017;72(2):177–182. - PubMed
-
- Alghamdi M. Familial Mediterranean fever, review of the literature. Clin Rheumatol. 2017;36(8):1707–1713. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
