

Promoting Angiogenesis in Oxidative Diabetic Wound Microenvironment Using a Nanozyme-Reinforced Self-Protecting Hydrogel
- PMID: 30937375
- PMCID: PMC6439452
- DOI: 10.1021/acscentsci.8b00850
Promoting Angiogenesis in Oxidative Diabetic Wound Microenvironment Using a Nanozyme-Reinforced Self-Protecting Hydrogel
Abstract
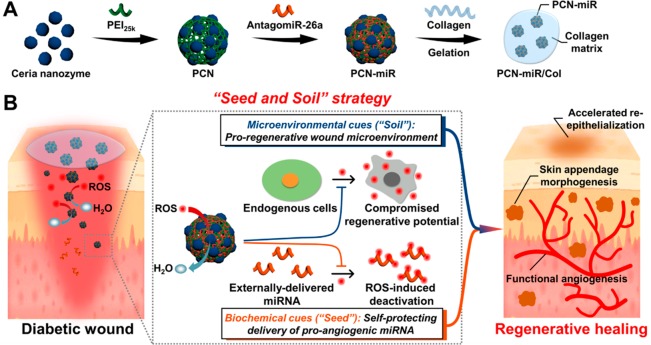
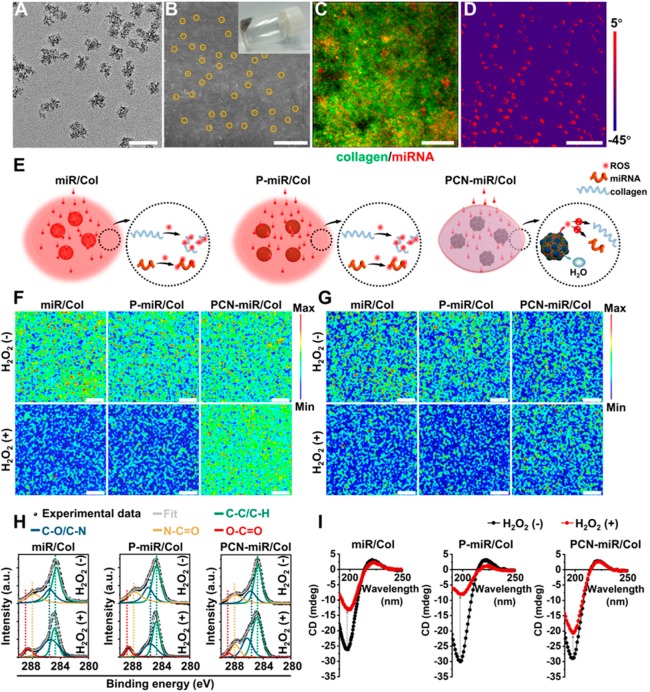
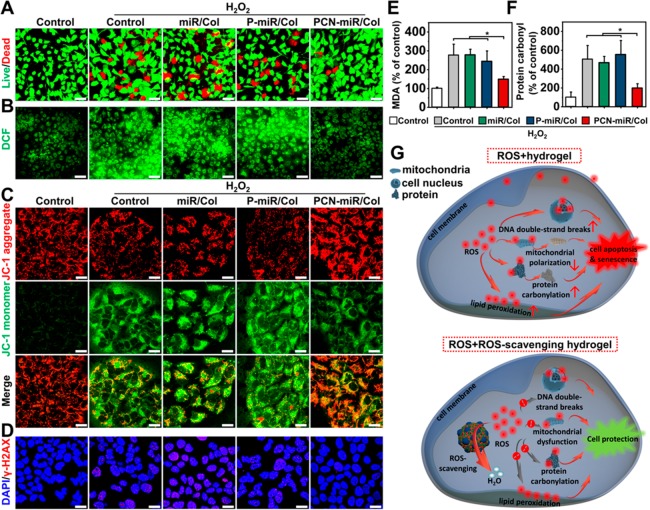
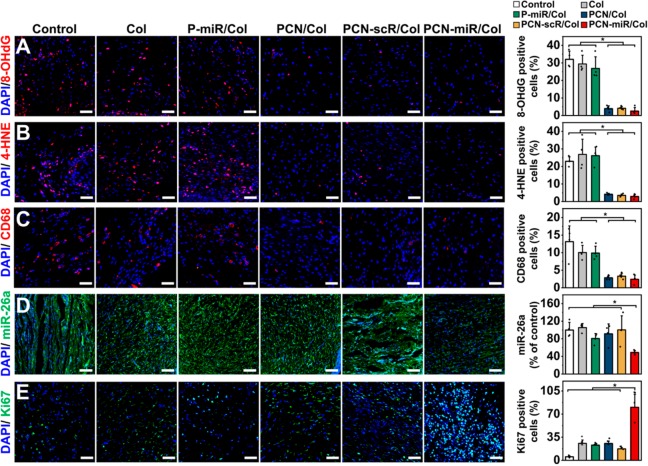
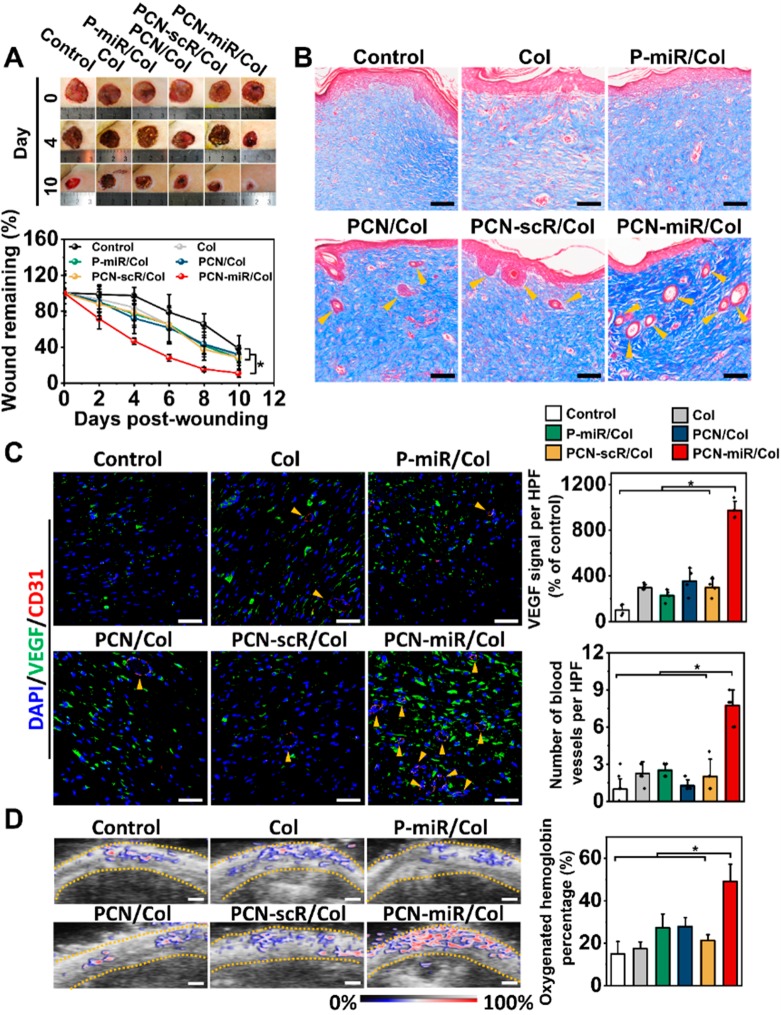
Impaired diabetic wound healing represents a devastating and rapidly growing clinical problem associated with high morbidity, mortality, and recurrence rates. Engineering therapeutic angiogenesis in the wounded tissue is critical for successful wound healing. However, stimulating functional angiogenesis of the diabetic wound remains a great challenge, due to the oxidative damage and denaturation of bio-macromolecule-based angiogenic agents in the oxidative diabetic wound microenvironment. Here, we present a unique "seed-and-soil" strategy that circumvents the limitation by simultaneously reshaping the oxidative wound microenvironment into a proregenerative one (the "soil") and providing proangiogenic miRNA cues (the "seed") using an miRNA-impregnated, redox-modulatory ceria nanozyme-reinforced self-protecting hydrogel (PCN-miR/Col). The PCN-miR/Col not only reshapes the hostile oxidative wound microenvironment, but also ensures the structural integrity of the encapsulated proangiogenic miRNA in the oxidative microenvironment. Diabetic wounds treated with the PCN-miR/Col demonstrate a remarkably accelerated wound closure and enhanced quality of the healed wound as featured by highly ordered alignment of collagen fiber, skin appendage morphogenesis, functional new blood vessel growth, and oxygen saturation.
Conflict of interest statement
The authors declare no competing financial interest.
Figures
References
-
- Duscher D.; Neofytou E.; Wong V. W.; Maan Z. N.; Rennert R. C.; Inayathullah M.; Januszyk M.; Rodrigues M.; Malkovskiy A. V.; Whitmore A. J.; et al. Transdermal deferoxamine prevents pressure-induced diabetic ulcers. Proc. Natl. Acad. Sci. U. S. A. 2015, 112, 94–99. 10.1073/pnas.1413445112. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources