

Patient preferences for whole-body MRI or conventional staging pathways in lung and colorectal cancer: a discrete choice experiment
- PMID: 30937589
- PMCID: PMC6554244
- DOI: 10.1007/s00330-019-06153-4
Patient preferences for whole-body MRI or conventional staging pathways in lung and colorectal cancer: a discrete choice experiment
Abstract
Objectives: To determine the importance placed by patients on attributes associated with whole-body MRI (WB-MRI) and standard cancer staging pathways and ascertain drivers of preference.
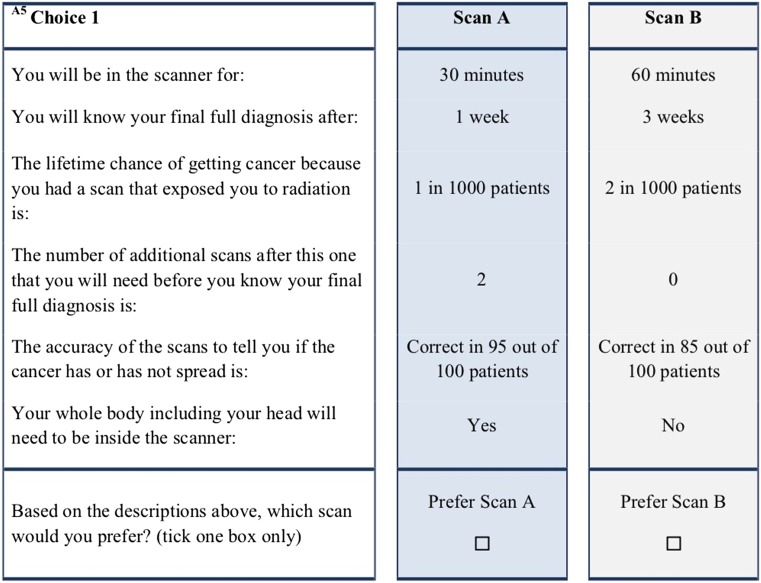
Methods: Patients recruited to two multi-centre diagnostic accuracy trials comparing WB-MRI with standard staging pathways in lung and colorectal cancer were invited to complete a discrete choice experiment (DCE), choosing between a series of alternate pathways in which 6 attributes (accuracy, time to diagnosis, scan duration, whole-body enclosure, radiation exposure, total scan number) were varied systematically. Data were analysed using a conditional logit regression model and marginal rates of substitution computed. The relative importance of each attribute and probabilities of choosing WB-MRI-based pathways were estimated.
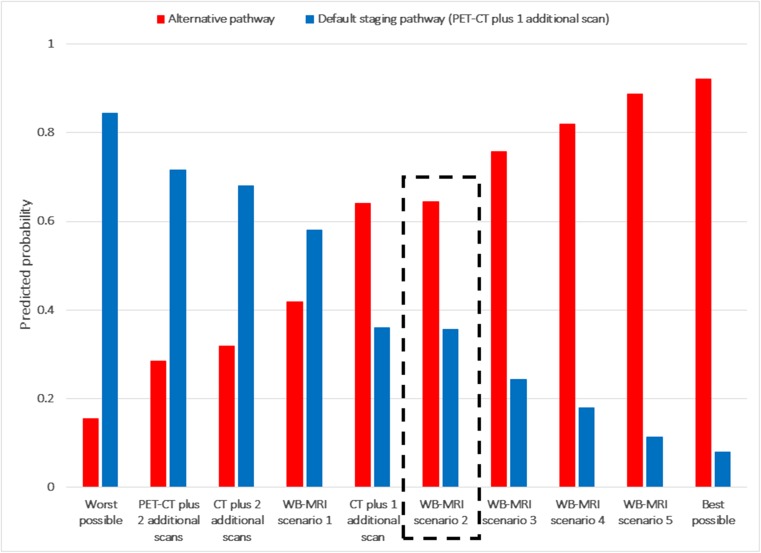
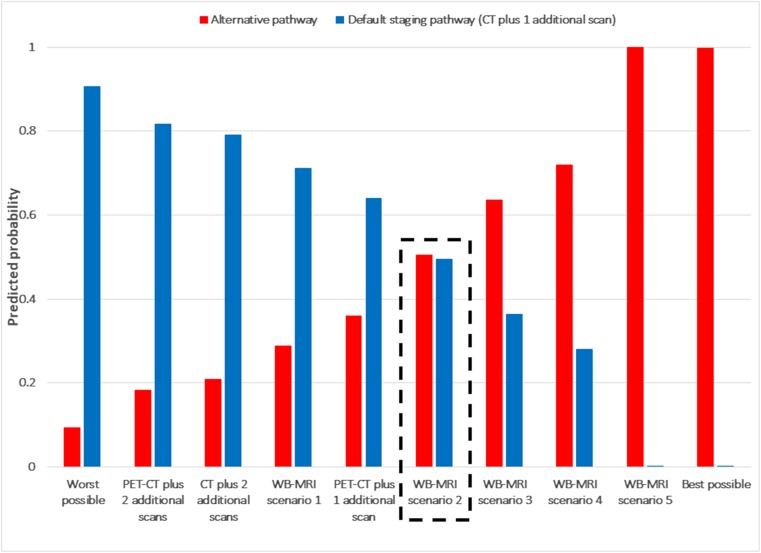
Results: A total of 138 patients (mean age 65, 61% male, lung n = 72, colorectal n = 66) participated (May 2015 to September 2016). Lung cancer patients valued time to diagnosis most highly, followed by accuracy, radiation exposure, number of scans, and time in the scanner. Colorectal cancer patients valued accuracy most highly, followed by time to diagnosis, radiation exposure, and number of scans. Patients were willing to wait 0.29 (lung) and 0.45 (colorectal) weeks for a 1% increase in pathway accuracy. Patients preferred WB-MRI-based pathways (probability 0.64 [lung], 0.66 [colorectal]) if they were equivalent in accuracy, total scan number, and time to diagnosis compared with a standard staging pathway.
Conclusions: Staging pathways based on first-line WB-MRI are preferred by the majority of patients if they at least match standard pathways for diagnostic accuracy, time to diagnosis, and total scan number.
Key points: • WB-MRI staging pathways are preferred to standard pathways by the majority of patients provided they at least match standard staging pathways for accuracy, total scan number, and time to diagnosis. • For patients with lung cancer, time to diagnosis was the attribute valued most highly, followed by accuracy, radiation dose, number of additional scans, and time in a scanner. Preference for patients with colorectal cancer was similar. • Most (63%) patients were willing to trade attributes, such as faster diagnosis, for improvements in pathway accuracy and reduced radiation exposure.
Keywords: Cancer; Magnetic resonance imaging; Patient preference; Positron emission tomography; Tomography, X-ray computed.
Conflict of interest statement
Stuart Taylor is a research consultant to Robarts.
Figures

References
-
- Usuda K, Sagawa M, Maeda S, et al. Diagnostic performance of whole-body diffusion-weighted imaging compared to PET-CT plus brain MRI in staging clinically resectable lung cancer. Asian Pac J Cancer Prev. 2016;17:2775–2780. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
