

Regressed coronary ostial stenosis in a young female with Takayasu arteritis: a case report
- PMID: 30940076
- PMCID: PMC6446325
- DOI: 10.1186/s12872-019-1066-7
Regressed coronary ostial stenosis in a young female with Takayasu arteritis: a case report
Abstract
Background: Takayasu arteritis is a rare systemic vasculitis, which affects the aorta and its major branches, especially in young females. Diagnosis and treatment for Takayasu arteritis with coronary stenosis are important to prevent fatal complications. Immunosuppressive treatment such as corticosteroid is a common treatment for this condition. However, the effects of immunosuppressive treatment on inflammatory coronary stenosis caused by Takayasu arteritis remains unknown.
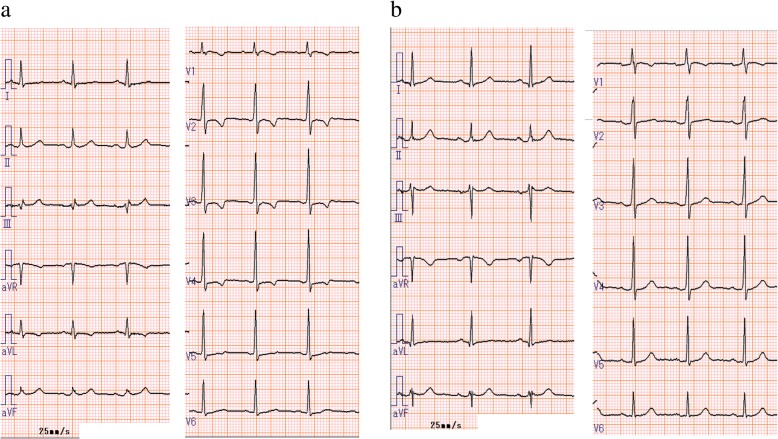
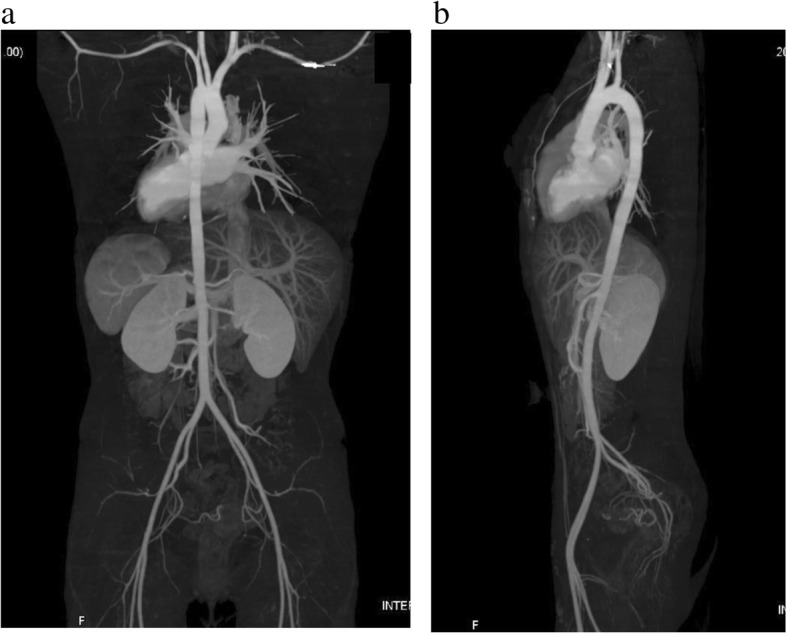
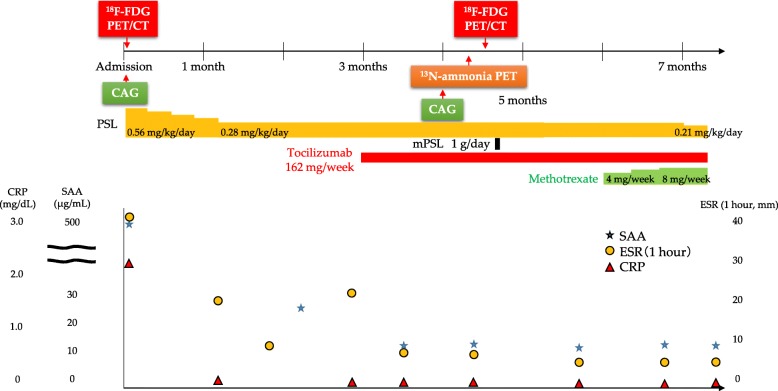
Case presentation: An 18-year-old female had chest oppression on effort and was referred to our hospital due to ST-segment depression in I, aVL, and V2-4 on electrocardiogram. Coronary angiography showed severe stenosis in the ostium of both the left main trunk and the right coronary artery. 18F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography showed isolated inflammation of the aortic root. She was diagnosed with Takayasu arteritis and treated with combined immunosuppressive treatment with corticosteroid and tocilizumab, which decreased the FDG uptake in the aortic root. Four months after initiation of the immunosuppressive treatment, coronary angiography showed regression of the coronary ostial stenosis. Coronary artery bypass surgery was considered, but the patient rejected invasive revascularization for coronary artery disease. She did not have chest oppression or ST-segment depression after the immunosuppressive treatment. She had no cardiac events for 6 months after discharge.
Conclusions: We described regressed coronary ostial stenosis in a young female patient with Takayasu arteritis. Immunosuppressive treatment might have a favorable effect on coronary ostial stenosis in Takayasu arteritis.
Keywords: 18F-fluorodeoxyglucose positron emission tomography/computed tomography; Case report; Coronary ostial stenosis; Regression; Takayasu arteritis; Tocilizumab.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the ethics committee of Fukushima Medical University and written informed consent was provided by the patient.
Consent for publication
Consent for publication was obtained by the patient in written form.
Competing interests
Tetsuro Yokokawa belongs to a department supported by Actelion Pharmaceuticals Japan Ltd. Akiomi Yoshihisa belongs to a department supported by Fukuda Denshi Co, Ltd. These companies are not associated with the contents of this study. No other authors have competing interests associated with this study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
-
- Amano J, Suzuki A. Coronary artery involvement in Takayasu's arteritis. Collective review and guideline for surgical treatment. J Thorac Cardiovasc Surg. 1991;102:554–560. - PubMed
-
- Nagata S. Present state of autopsy cases of Takayasu’s arteritis (aortitis syndrome) in Japan. J Jpn Coll Angiol. 1990;30:1303–1308.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
