

Patient-reported advantages and disadvantages of peritoneal dialysis: results from the PDOPPS
- PMID: 30940103
- PMCID: PMC6446371
- DOI: 10.1186/s12882-019-1304-3
Patient-reported advantages and disadvantages of peritoneal dialysis: results from the PDOPPS
Abstract
Background: Patient-reported measures are increasingly recognized as important predictors of clinical outcomes in peritoneal dialysis (PD). We sought to understand associations between patient-reported perceptions of the advantages and disadvantages of PD and clinical outcomes.
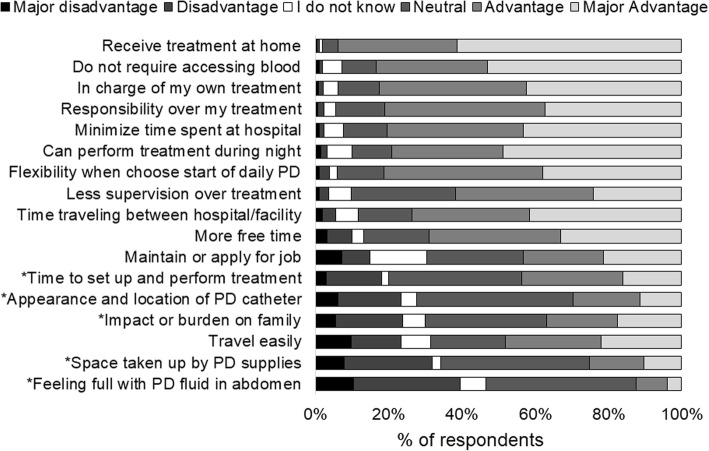
Methods: In this cohort study, 2760 PD patients in the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS) completed a questionnaire on their PD experience, between 2014 and 2017. In this questionnaire, PDOPPS patients rated 17 aspects of their PD experience on a 5-category ordinal scale, with responses scored from - 2 (major disadvantage) to + 2 (major advantage). An advantage/disadvantage score (ADS) was computed for each patient by averaging their response scores. The ADS, along with each of these 17 aspects, were used as exposures. Outcomes included mortality, transition to hemodialysis (HD), patient-reported quality of life (QOL), and depression. Cox regression was used to estimate associations between ADS and mortality, transition to HD, and a composite of the two. Logistic regression with generalized estimating equations was used to estimate cross-sectional associations of ADS with QOL and depression.
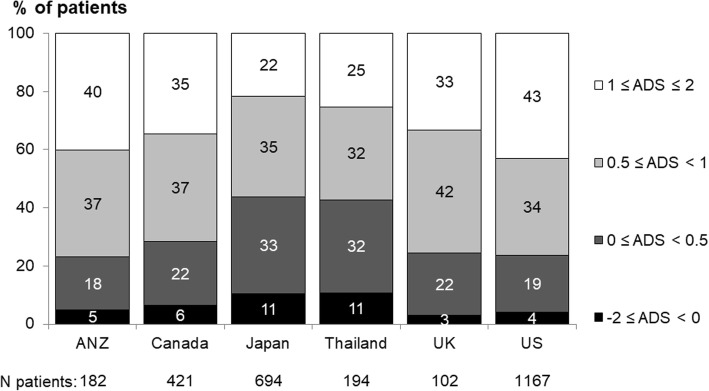
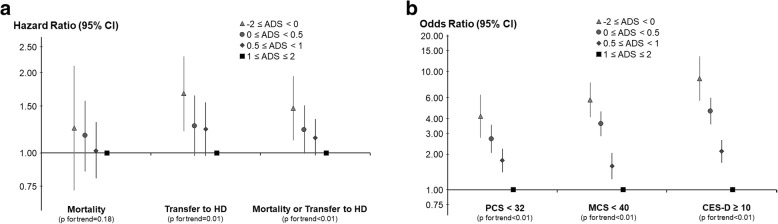
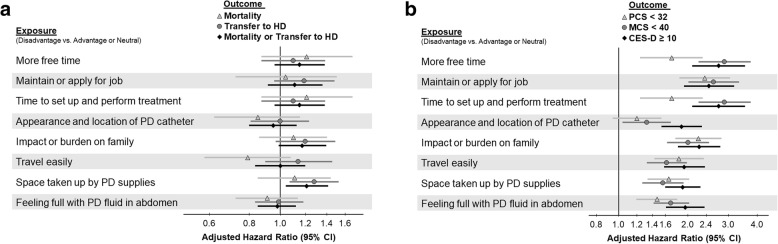
Results: While 7% of PD patients had an ADS < 0 (negative perception of PD), 59% had an ADS between 0 and < 1 (positive perception), and 34% had an ADS ≥1 (very positive perception). Minimal association was observed between mortality and the ADS. Compared with a very positive perception, patients with a negative perception had a higher transition rate to HD (hazard ratio [HR] = 1.67; 95% confidence interval [CI]: 1.21, 2.30). Among individual items, "space taken up by PD supplies" was commonly rated as a disadvantage and had the strongest association with transition to HD (HR = 1.28; 95% CI 1.07, 1.53). Lower ADS was strongly associated with worse QOL rating and greater depressive symptoms.
Conclusions: Although patients reported a generally favorable perception of PD, patient-reported disadvantages were associated with transition to HD, lower QOL, and depression. Strategies addressing these disadvantages, in particular reducing solution storage space, may improve patient outcomes and the experience of PD.
Keywords: Depression; Patient selection; Patient-reported measures; Peritoneal dialysis; Quality of life; Surveys and questionnaires; Technique survival.
Conflict of interest statement
Ethics approval and consent to participate
As detailed under Methods: The PDOPPS was approved by a central institutional review board (IRB) in the US, with IRB study approval and patient consent obtained for each patient, as required by national and local ethics committee regulations.
Data from US patients receiving care at large dialysis organization (LDO) sites are imported from electronic health records; data from non-LDO US and non-US patients were obtained from manual medical chart abstraction and entered into a web-based data collection tool.
Patient-reported advantages and disadvantages of PD were collected using the PDOPPS PQ, which was mailed to each facility participating in the PDOPPS. All patients who were consented into the PDOPPS were then asked by the facility’s research coordinator or nurse to complete the questionnaire at the time the patient visited the facility for their routine visit. Completing this was voluntary, and patients were able to participate in the study without completing the questionnaire.
Consent for publication
Please see above section, “Ethics Approval and Consent to Participate.”
Competing interests
Jeff Perl has received speaking honoraria from Baxter Healthcare, Fresenius Medical Care, Davita Healthcare Partners, and consulting fees from Baxter Healthcare, Fresenius Medical Care, as well as unrestricted research support from Baxter Healthcare and salary support from Arbor Research Collaborative for Health.
David Johnson has previously received consultancy fees, research grants, travel sponsorships and speaker’s honoraria from Baxter Healthcare and Fresenius Medical Care. He has also received consultancy fees from Astra Zeneca and travel sponsorships from Amgen. He is a current recipient of an Australian National Health and Medical Research Council Practitioner Fellowship.
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
