

Individualized penetrating keratoplasty using edge-trimmed glycerol-preserved donor corneas for perforated corneal ulcers
- PMID: 30940116
- PMCID: PMC6444435
- DOI: 10.1186/s12886-019-1091-4
Individualized penetrating keratoplasty using edge-trimmed glycerol-preserved donor corneas for perforated corneal ulcers
Abstract
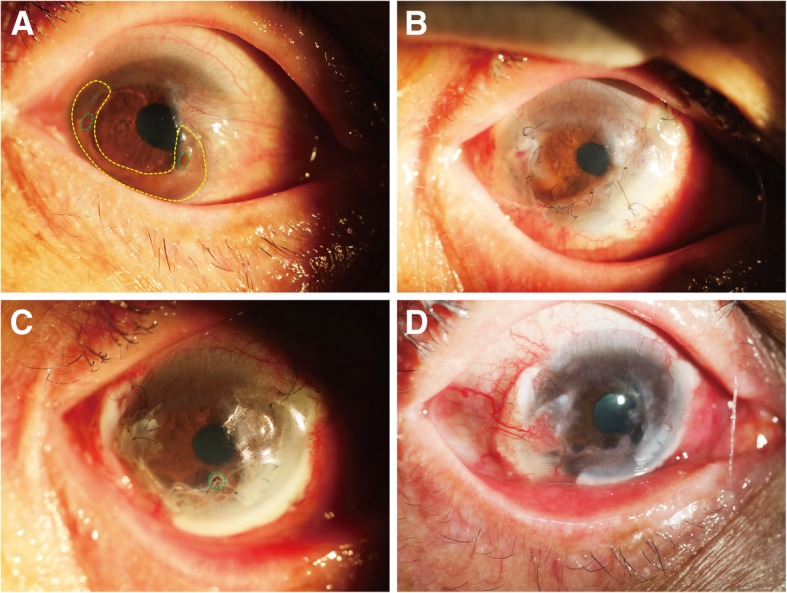
Purpose: To report a surgical technique and the surgical outcomes of individualized penetrating keratoplasty (PK) using edge-trimmed glycerol-preserved donor corneas for perforated corneal ulcers.
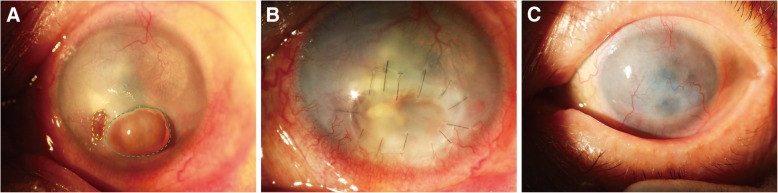
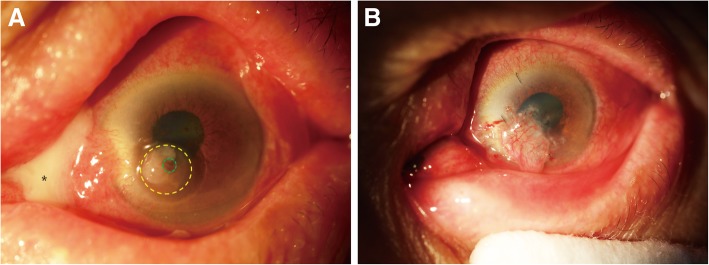
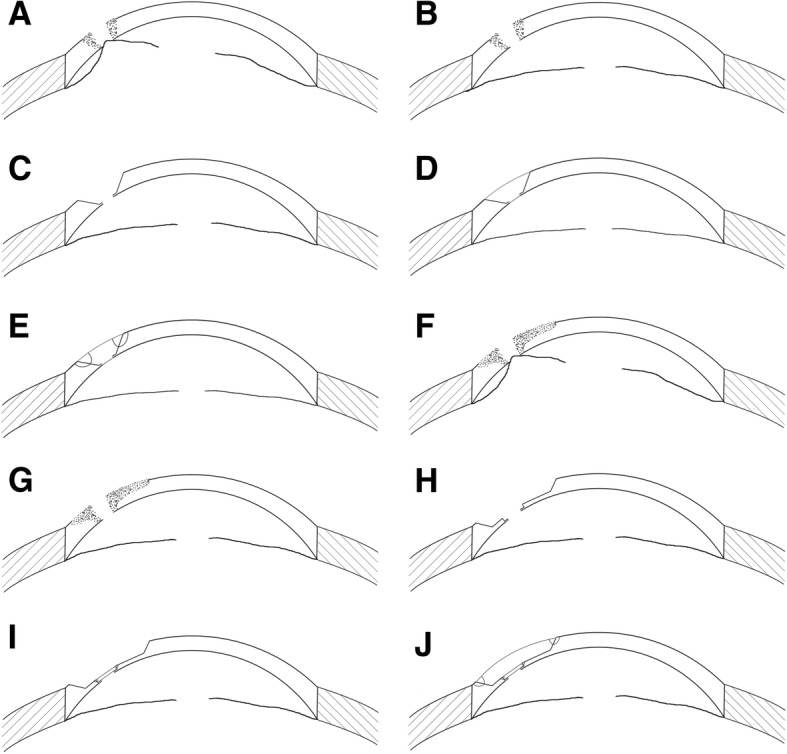
Methods: Fourteen perforated eyes from 14 patients who underwent individualized PK using edge-trimmed glycerol-preserved donor corneas, were included in the retrospective study. The perforations were mainly 1-2 mm in size except for one that was 2.5 × 4 mm. Three patients were treated with PK; one patient was treated with PK and a conjunctival flap; ten patients who had large ulcer areas were treated with PK combined with lamellar keratoplasty (LK). Donor corneas were preserved in sterile pure glycerol at - 80 °C. Corneal grafts were specially edge-trimmed to match the perforation, and then sutured onto the recipient bed avoiding the visual axis.
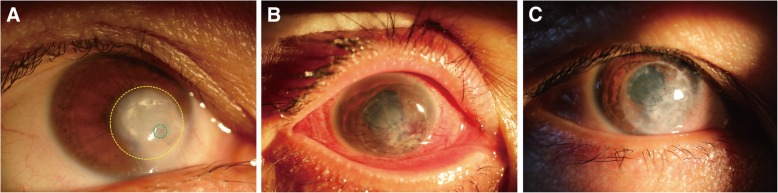
Results: All 14 patients recovered anatomical integrity without reinfections of the treated eyes. All patients had improved graft transparency and uncorrected visual acuity after surgery. Among them, four patients suffered from short-term postoperative complications and recovered quickly; four patients suffered from long-term postoperative complications, of them, one was performed further treatment.
Conclusion: After individualized PK using glycerol-preserved donor corneas, all perforated corneal ulcers were stably controlled by the end of the follow-up period. This modified surgical technique can be a potential treatment choice for patients with perforated corneal ulcers.
Keywords: Cornea; Corneal perforation; Individualized penetrating keratoplasty; Preserved.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Tongji Hospital, Tongji University School of Medicine, and adhered to the tenets of the Declaration of Helsinki. Due to the retrospective nature of the study, informed consent was waived.
Consent for publication
Written informed consent was obtained from the patients for publication of this article and any accompanying images. Copies of the written consents are available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
