Characterizing advanced Parkinson's disease: OBSERVE-PD observational study results of 2615 patients
- PMID: 30940119
- PMCID: PMC6444751
- DOI: 10.1186/s12883-019-1276-8
Characterizing advanced Parkinson's disease: OBSERVE-PD observational study results of 2615 patients
Abstract
Background: There are currently no standard diagnostic criteria for characterizing advanced Parkinson's disease (APD) in clinical practice, a critical component in determining ongoing clinical care and therapeutic strategies, including transitioning to device-aided treatment. The goal of this analysis was to determine the proportion of APD vs. non-advanced PD (non-APD) patients attending specialist PD clinics and to demonstrate the clinical burden of APD.
Methods: OBSERVE-PD, a cross-sectional, international, observational study, was conducted with 2615 PD patients at 128 movement disorder centers in 18 countries. Motor and non-motor symptoms, activities of daily living, and quality-of-life end points were assessed. The correlation between physician's global assessment of advanced PD and the advanced PD criteria from a consensus of an international group of experts (Delphi criteria for APD) were evaluated.
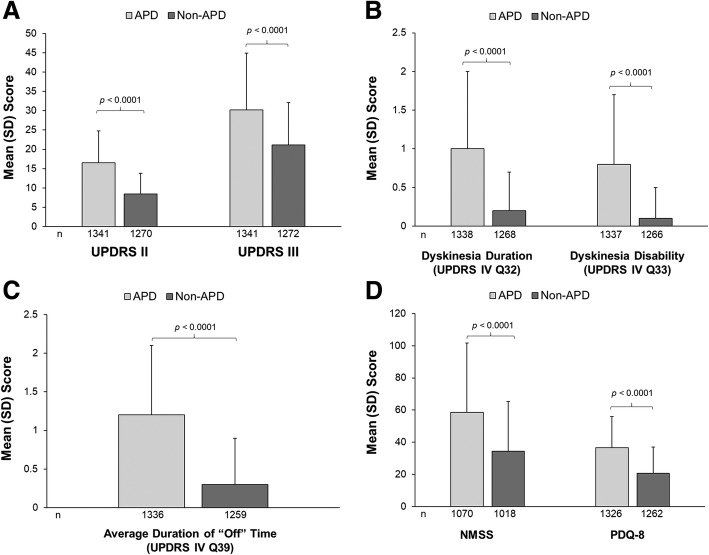
Results: According to physician's judgment, 51% of patients were considered to have APD. There was a moderate correlation between physician's judgment and Delphi criteria for APD (K = 0.430; 95% CI 0.406-0.473). Activities of daily living, motor symptom severity, dyskinesia duration/disability, "Off" time duration, non-motor symptoms, and quality-of-life scores were worse among APD vs. non-APD patients (p < 0.0001 for all). APD patients (assessed by physicians) had higher disease burden by motor and non-motor symptoms compared with non-APD patients and a negative impact on activities of daily living and quality of life.
Conclusions: These findings aid in identifying standard APD classification parameters for use in practicing physicians. Improvements in identification of APD patients may be particularly relevant for optimizing treatment strategies including transitioning to device-aided treatment.
Keywords: Advanced Parkinson’s disease; Device-aided treatment; Quality of life.
Conflict of interest statement
Ethics approval and consent to participate
To be included in the study, patients had to sign an authorization form to disclose personal health information and provided written informed consent. The study was approved by local ethics committees and performed according to the International Conference on Harmonization and Good Clinical Practice requirements, in accord with the principles of the Declaration of Helsinki. The local ethics committees that provided approval included those in Austria (Ethik Kommission des Landes Oberösterreich, Ethikkommission der Medizinischen Universität Innsbruck, Ethik Kommission des Bundeslandes Niederösterreichs), in Belgium (Universitair Ziekenhuis Antwerpen), in Canada (REB of Centre intégré de santé et de services sociaux de Chaudière-Appalach [MSSS pour les centres du Québec], Health Research Ethics Boards [UofA], Western University Health Science REB [HSREB], MSSS [authorized by MUHC], Ottawa Health Science Network REB, Conjoint Health Research Ethics Board of the University of Calgary, Queen’s University Health Sciences & Affiliated teaching hospitals REB [HSREB], University Health Network REB, IRB Services [Advarra], REB Horizon Health Network, MSSS [authorized by JGH], IRB Services [Advarra]), in Switzerland (Ethikkommission Ostschweiz Kantonsspital), in Germany (Ethikkommission der Universität zu Köln, Ethikkommission der Landesärztekammer Brandenburg, Ethikkommission Ärztekammer Niedersachsen, Ethikkommission der Ländesärztekammer Thüringen, Ethik-Kommission Landesärztekammer Baden-Württemberg, Ethik-Kommission Albert-Ludwigs-Universität Freiburg, Ethik-Kommission der Ärztekammer Berlin, Ethikkommission Ärztekammer Nordrhein, Ethik-Kommission der Bayerischen Landesärztekammer, Ethik-kommission der Ärztekammer Hamburg, Ethikkommission Ärztekamer Niedersachsen, Ethik-Kommission Rheinische Friedrich-Wilhelms-Universität Medizinische Fakultät, Ethikkommission Ärztekammer Sachsen-Anhalt, Ethikkommission Ärztekammer Niedersachsen, Ethikkommission Ärztekammer Nordrhein), in Greece (Ethics Committee of General Hospital of Thessaloniki “G. Papanikolaou”, Ethics Committee of General Hospital of Thessaloniki “Papageorgiou”, Ethics Committee of 251 Airforce General Hospital, Ethics Committee of Naval Hospital of Athens, Ethics Committee of University General Hospital “Attikon”, Ethics Committee of University General Hospital of Heraklion, Ethics Committee of University General Hospital of Patras, Ethics Committee of Mediterraneo Hospital, Ethics Committee of University General Hospital of Alexandroupoli, Ethics Committee of HYGEIA Hospital, Ethics Committee of General Hospital of Athens “G. Gennimatas”, Ethics Commmittee of University General Hospital of Thessaloniki “Axepa”, Ethics Committee of University General Hospital of Ioannina, Ethics Committee of 417 Nursing Institution of Participial Army Fund [NIMTS]), in Ireland (Education and Research Committee St Vincent’s University Hospital, Joint Research Ethics Committee SJH/AMNCH, Clinical Research Ethics Committee of the Cork Teaching Hospitals, Galway research ethics committee), in Israel (E. Wolfson Medical Center Helsinki Committee, IRB Committee Sheba Medical Center Israel, Tel Aviv Sourasky Medical Center Institutional Review Board, Ethics committee of Rabin Medical Center), in Italy (Comitato Etico delle Aziende Sanitarie dell’Umbria di Perugia, Comitato Etico Regional [CER] delle Marche c/o AUO Ospedali Riuniti, Comitato Etico AOU di Cagliari, Comitato Etico Indipendente Azienda Ospedaliero Universitaria Policlinico Consorziale di Bari, Comitato Etico Interaziendale AOU Città della Salute e della Scienza di Torino AO Ordine Mauriziano – ASL TO1, Comitato Etico Interaziendale della Provincia di Messina AOU Policlinico “G Martino”, Comitato Etico Area Vasta Centro c/o AOU Careggi, Comitato Etico Indipendente dell’Azienda Ospedaliera Universitaria Policlinico Tor Vergata di Roma, Comitato Etico Seconda Università degli Studi di Napoli Azienda Ospedaliera Universitaria SUN-AORN “Ospedali dei Colli”), in Turkey (Kocaeli University Medical Faculty Ethics Committee), in the Czech Republic (Ethics Committee of the General Hospital of Charles University in Prague, Ethics Committee of the St Anna Hospital of Masaryk University in Brno), in Slovakia (the local legislation valid at that time of 2015 did not impose an obligation to approve epidemiological observational studies by the ethics committee; therefore, the opinions of the two ethics committees in the Czech Republic can be used to comply with the ethical principles in both countries), in Russia (Advisory council on ethics St Petersburg state budgetary healthcare institution city hospital No 40, Ethics committee of the federal state budgetary institution state research center, Independent Interdisciplinary Committee for Ethical Review of Clinical Studies [125468, Moscow, Leningradskiy prospect 51]), in Romania (National Commission of Bioethics [Comisia Nationala de Bioetica a Medicamentului si a Dispozitivelor Medicale]), in Hungary (Ethics committees of the Medical Research Council of Hungary [ETT] Egészségügyi Tudományos Tanács Klinikai Farmakológiai Etikai Bizottsága), in Slovenia (Republic of Slovenia Medical Ethics Committee, Institute of Clinical Neurophysiology, University Medical Centre Ljubljana [Komisija Republike Slovenije Za Medicinsko Etiko]), in Croatia (Drug Committee of Clinical Hospital Center Zagreb [Povjerenstvo za lijekove Kliničkog Bolničkog Centra Zagreb], Drug Committee of Clinical Hospital Center Osijek [Povjerenstvo za lijekove Kliničkog Bolničkog Centra Osijek], Drug Committee of Clinical Hospital Center Split [Povjerenstvo za lijekove Kliničkog Bolničkog Centra Split]), and Australia (Belberry Human Research Ethics Committee, Royal Brisbane and Women’s hospital human research ethics committee).
Consent for publication
Not applicable.
Competing interests
The authors report no direct conflict of interest related to the work on this manuscript. Full financial disclosure is provided as follows. A Fasano was a study investigator and has served as an advisor for AbbVie, Inc.; consultant for UCB pharma, Medtronic, Boston Scientific, Ipsen, Sunovion, and AbbVie, Inc. He has received research support from Medtronic, Boston Scientific, University of Toronto, Michael J. Fox Foundation for Parkinson’s Research, and honoraria from UCB pharma, Medtronic, Novartis, Chiesi, Boston Scientific, AbbVie, Inc., Ipsen, Sunovion, and Teva for serving as a speaker. VSC Fung receives a salary from NSW Health. He has received unrestricted research grants from AbbVie and Merz, is on advisory boards and/or has received travel grants from AbbVie, Allergan, Cavion, Ipsen, Merz, Praxis, Seqirus, Stada, Teva, and UCB, and receives royalties from Health Press Ltd. L Lopiano was a study investigator and received research support from University of Turin and honoraria and travel grants for serving as a consultant and speaker for AbbVie, Inc., UCB, and Zambon. B Elibol was a study investigator and has served as a local advisor for AbbVie, Inc. and has received honoraria from AbbVie, Inc. for serving as a speaker. IG Smolentseva was a study investigator. K Seppi has received consultancy fees from Teva, UCB, Lundbeck, AOP Orphan Pharmaceuticals AG, Roche, Grunenthal, and AbbVie. He has also received honoraria from the International Parkinson and Movement Disorders Society, research grants from FWF Austrian Science Fund, Michael J Fox Foundation, and the International Parkinson and Movement Disorder Society, outside the submitted work. A Takáts was a study investigator and has served as an advisor for AbbVie, Inc. She has also served as a consultant for UCB pharma, Ever pharma, TEVA, and AbbVie, Inc., and has received honoraria from UCB, MERZ, AbbVie, Inc., and Teva for serving as speaker. Z Pirtosek was a study investigator and has received compensation from AbbVie, Inc., for speaker-related activities. K Onuk, JC Parra, L Bergmann, K Sail, and Y Jalundhwala are employees of AbbVie, Inc., and may hold corporate stock or stock options.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures