

Sensitivity and specificity of routine diagnostic work-up for tuberculosis in lung clinics in Yogyakarta, Indonesia: a cohort study
- PMID: 30940123
- PMCID: PMC6444523
- DOI: 10.1186/s12889-019-6658-8
Sensitivity and specificity of routine diagnostic work-up for tuberculosis in lung clinics in Yogyakarta, Indonesia: a cohort study
Abstract
Background: Establishing a correct diagnosis is challenging. We aimed to investigate the sensitivity and specificity of routine tuberculosis (TB) diagnostic work-up in lung clinics in Indonesia, a country with the third highest TB burden and the second highest gap between notifications of TB cases and the best estimate of incident cases in the world.
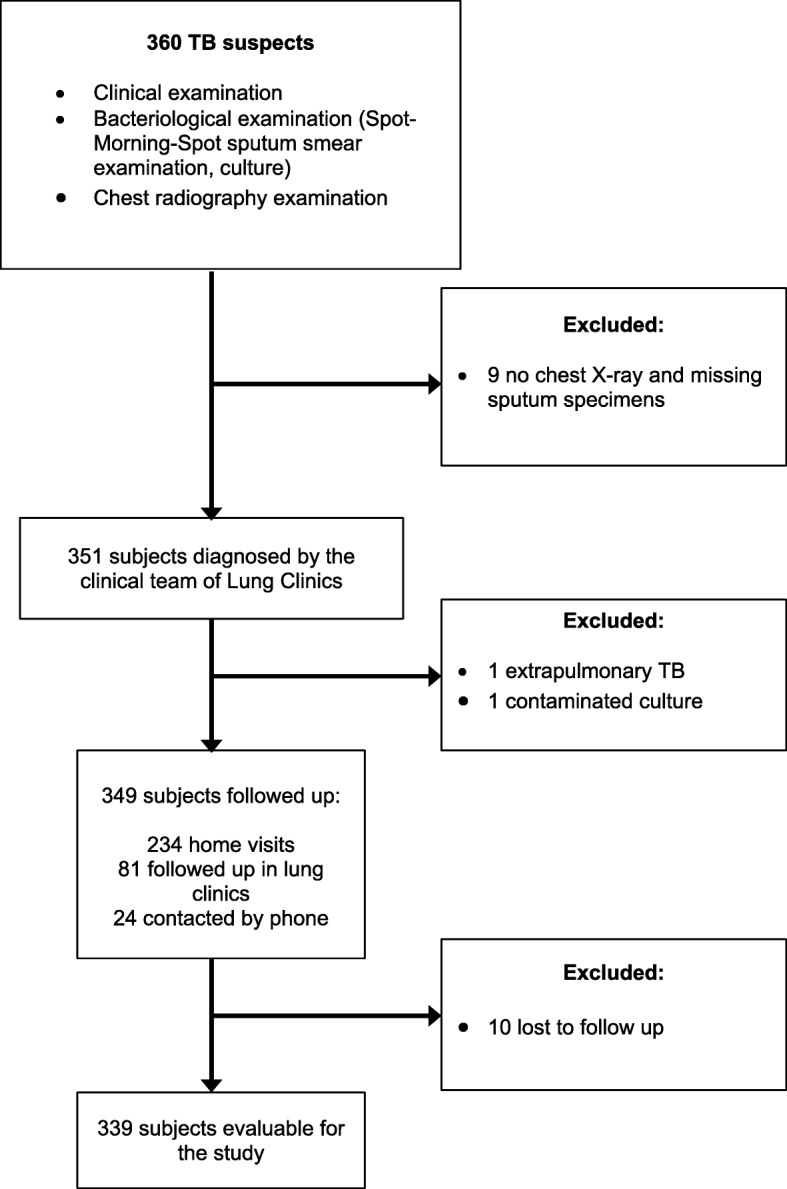
Methods: In the lung clinics of the Province of Yogyakarta, Indonesia, we recruited all consecutive patients with symptoms suggesting TB, aged ≥18 years. Routine TB examination consisted of clinical evaluation, sputum smear microscopy, and chest radiography. For research purposes, we added sputum culture, Human Immunodeficiency Virus (HIV) testing, and follow-up for 1.5 years or 2.5 years if culture results disagreed with the initial clinical diagnosis. The initial diagnosis was considered incorrect if patients did not respond to treatment. We calculated sensitivity and specificity of the TB routine examination using culture and a composite reference standard (CRS - a combination of routine examination, culture, and follow-up) as the reference standards. All analyses were conducted with IBM SPSS Statistics 25 (IBM Corp., Armonk, NY, USA).
Results: Between 2013 and 2015, we included 360 participants, and 21 were excluded due to incomplete data. Among those analyzed, 115 were initially diagnosed with smear-positive TB, 12 with smear-negative TB, and 212 non-TB. In 15 study participants, the diagnosis was changed after median 45 (range: 14-870) days; 14 participants initially not diagnosed with TB were later diagnosed with TB, while one subject initially diagnosed with TB actually did not have TB. Compared with culture and CRS, TB routine examination had sensitivity of 85% (95%CI: 77-91) and 90% (95%CI: 84-94), and specificity of 86.3% (95%CI: 81-91) and 99.5% (95%CI: 97-100), respectively.
Conclusions: A combination of clinical evaluation with sputum microscopy and chest radiography provided high sensitivity and specificity in diagnosing TB in lung clinics; in only 4.4% the diagnosis was incorrect. There is a need to improve routine TB diagnostic work by using clinical evaluation, sputum smear microscopy, and chest radiography all together in other settings, such as in primary health centers.
Trial registration: NCT02219945 , clinicaltrials.gov . Registered 19 August 2014 (retrospectively registered).
Keywords: Culture; Diagnosis; Microscopy; Radiography; Sensitivity; Specificity; Tuberculosis.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
The study was conducted according to Helsinki Declaration 2013 and was approved by the institutional review board at Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia (KE/FK/859/EC). Written consent was informed, and all subjects provided their written consent before participation in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
-
- World Health Organization. Global Tuberculosis Report 2018. 2018.http://apps.who.int/iris/bitstream/handle/10665/274453/9789241565646-eng.... Accessed 27 Sep 2018.
-
- Kementerian Kesehatan Republik Indonesia. Pedoman Nasional Penanggulangan Tuberkulosis. 2014. https://puskespemda.net/download/pedoman-nasional-pengendalian-tuberkulo.... Accessed 20 Mar 2016.
-
- World Health Organization . Treatment of tuberculosis guidelines. 4 2010. - PubMed
-
- Davies PD, Pai M. The diagnosis and misdiagnosis of tuberculosis. Int J Tuberc Lung Dis. 2008;12(11):1226–1234. - PubMed
-
- Singh VK, Chandra S, Kumar S, Pangtey G, Mohan A, Guleria R. A common medical error: lung cancer misdiagnosed as sputum negative tuberculosis. Asian Pac J Cancer Prev. 2009;10(3):335–338. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
