

Impact of bleeding complications on length of stay and critical care utilization in cardiac surgery patients in England
- PMID: 30940172
- PMCID: PMC6444533
- DOI: 10.1186/s13019-019-0881-3
Impact of bleeding complications on length of stay and critical care utilization in cardiac surgery patients in England
Abstract
Background: Bleeding is a significant complication in cardiac surgery and is associated with substantial morbidity and mortality. This study evaluated the impact of bleeding on length of stay (LOS) and critical care utilization in a nationwide sample of cardiac surgery patients treated at English hospitals.
Methods: Retrospective, observational cohort study using linked English Hospital Episode Statistics (HES) and Clinical Practice Research Datalink (CPRD) records for a nationwide sample of patients aged ≥18 years who underwent coronary artery bypass graft (CABG), valve repair/replacement, or aortic operations from January 2010 through February 2016. The primary independent variables were in-hospital bleeding complications and reoperation for bleeding before discharge. Generalized linear models were used to quantify the adjusted mean incremental difference [MID] in post-procedure LOS and critical care days associated with bleeding complications, independent of measured baseline characteristics.
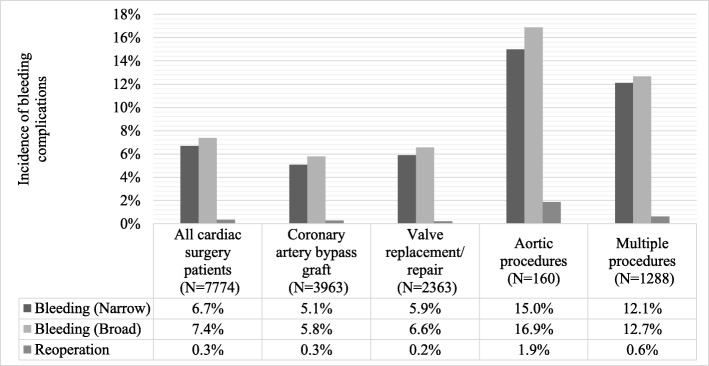
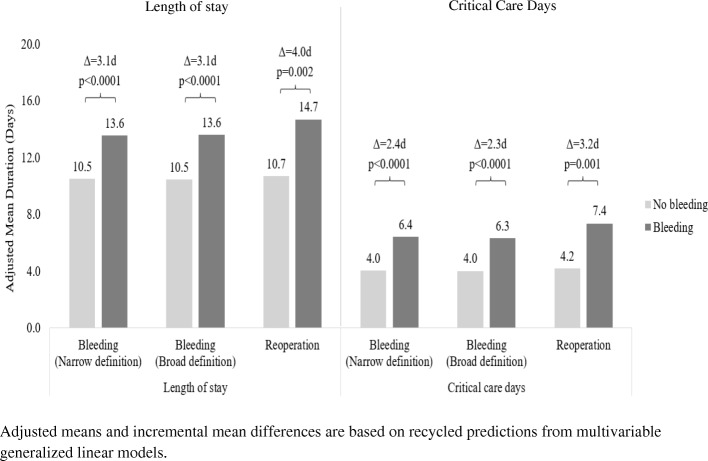
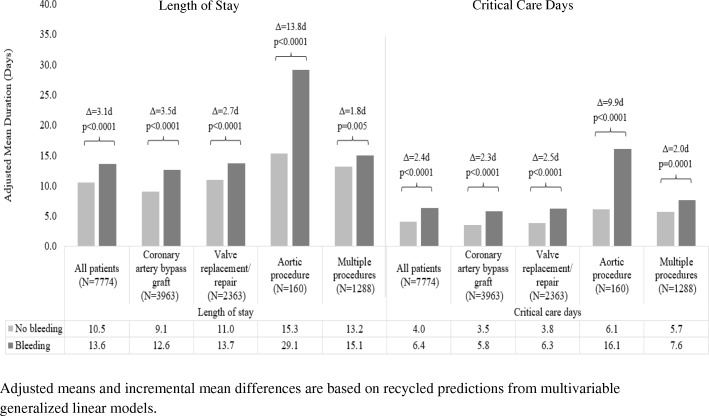
Results: The study included 7774 cardiac surgery patients (3963 CABG; 2363 valve replacement/repair; 160 aortic procedures; 1288 multiple procedures, primarily CABG+valve). Mean LOS was 10.7d, including a mean of 4.2d in critical care. Incidences of in-hospital bleeding complications and reoperation for bleeding were 6.7 and 0.3%, respectively. Patients with bleeding had longer LOS (MID: 3.1d; p < 0.0001) and spent more days in critical care (MID: 2.4d; p < 0.0001). Reoperation for bleeding was associated with larger increases in LOS (MID = 4.0d; p = 0.002) and days in critical care (MID = 3.2d; p = 0.001).
Conclusions: Among English cardiac surgery patients, in-hospital bleeding complications were associated with substantial increases in healthcare utilization. Increased use of evidence-based strategies to prevent and manage bleeding may reduce the clinical and economic burden associated with bleeding complications in cardiac surgery.
Keywords: Cardiac Surgical procedures; Complications; Costs and cost Analysis; Haemorrhage; Length of stay.
Conflict of interest statement
Ethics approval and consent to participate
The HES-APC and CPRD study data were de-identified and obtained under license from the UK Medicines and Healthcare Products Regulatory Agency (MHRA). Throughout the duration of the study, the data were stored on encrypted, password-protected servers to protect patient confidentiality. The study protocol (number 17_091R) was reviewed and approved by the Independent Scientific Advisory Committee for MHRA Database Research.
Consent for publication
Not applicable.
Competing interests
E. Ammann, S. Johnston, N. Jamous, S. Mistry, G. Gangoli, W. Danker, and K. Etter are employed by Johnson & Johnson. E. Ghosh is employed by Mu Sigma. Mu Sigma was paid by Johnson & Johnson to conduct the study. N. Al-Attar reports no disclosures.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Dacey LJ, Munoz JJ, Baribeau YR, Johnson ER, Lahey SJ, Leavitt BJ, et al. Reexploration for hemorrhage following coronary artery bypass grafting: incidence and risk factors. Northern New England cardiovascular disease study group. Arch Surg. 1998;133(4):442–447. doi: 10.1001/archsurg.133.4.442. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
