

Preoperative predictors of poor acute postoperative pain control: a systematic review and meta-analysis
- PMID: 30940757
- PMCID: PMC6500309
- DOI: 10.1136/bmjopen-2018-025091
Preoperative predictors of poor acute postoperative pain control: a systematic review and meta-analysis
Abstract
Objectives: Inadequate postoperative pain control is common and is associated with poor clinical outcomes. This study aimed to identify preoperative predictors of poor postoperative pain control in adults undergoing inpatient surgery.
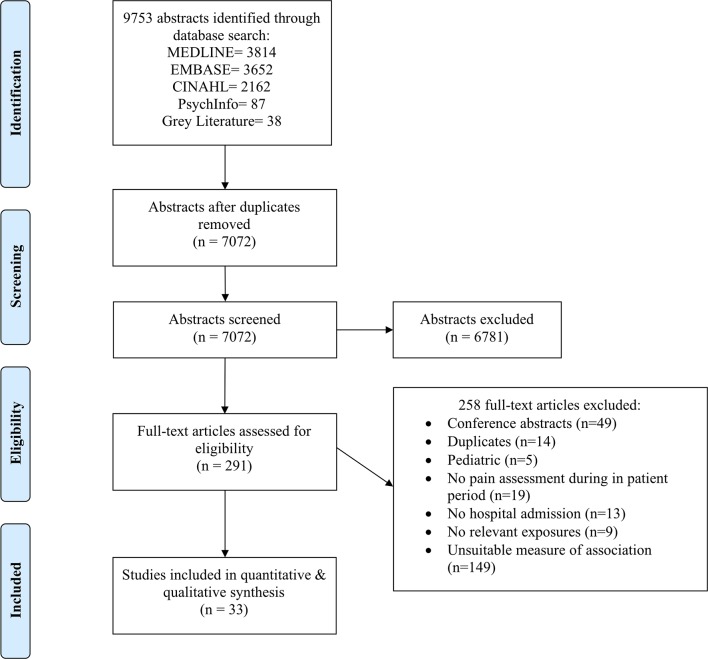
Design: Systematic review and meta-analysis DATA SOURCES: MEDLINE, Embase, CINAHL and PsycINFO were searched through October 2017.
Eligibility criteria: Studies in any language were included if they evaluated postoperative pain using a validated instrument in adults (≥18 years) and reported a measure of association between poor postoperative pain control (defined by study authors) and at least one preoperative predictor during the hospital stay.
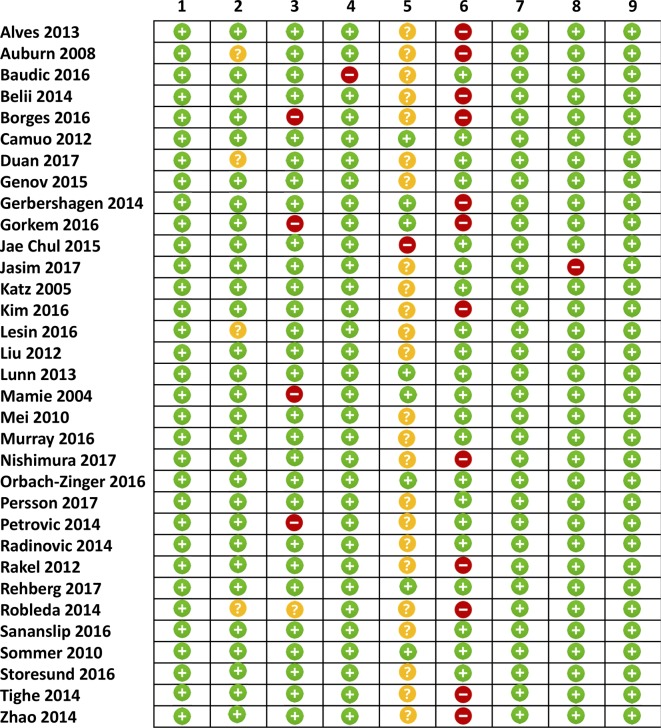
Data extraction and synthesis: Two reviewers screened articles, extracted data and assessed study quality. Measures of association for each preoperative predictor were pooled using random effects models.
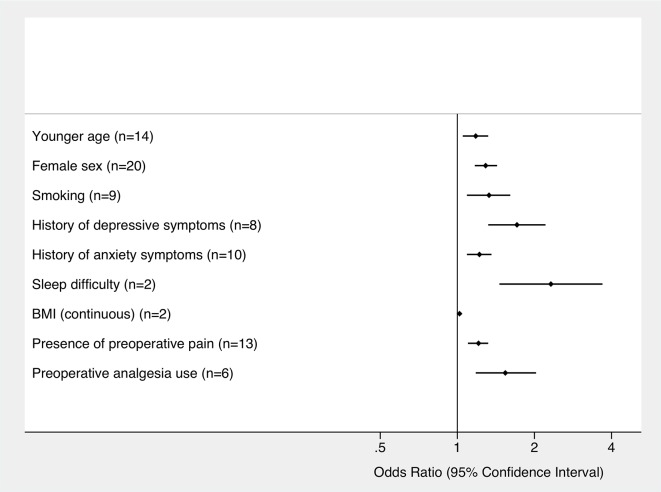
Results: Thirty-three studies representing 53 362 patients were included in this review. Significant preoperative predictors of poor postoperative pain control included younger age (OR 1.18 [95% CI 1.05 to 1.32], number of studies, n=14), female sex (OR 1.29 [95% CI 1.17 to 1.43], n=20), smoking (OR 1.33 [95% CI 1.09 to 1.61], n=9), history of depressive symptoms (OR 1.71 [95% CI 1.32 to 2.22], n=8), history of anxiety symptoms (OR 1.22 [95% CI 1.09 to 1.36], n=10), sleep difficulties (OR 2.32 [95% CI 1.46 to 3.69], n=2), higher body mass index (OR 1.02 [95% CI 1.01 to 1.03], n=2), presence of preoperative pain (OR 1.21 [95% CI 1.10 to 1.32], n=13) and use of preoperative analgesia (OR 1.54 [95% CI 1.18 to 2.03], n=6). Pain catastrophising, American Society of Anesthesiologists status, chronic pain, marital status, socioeconomic status, education, surgical history, preoperative pressure pain tolerance and orthopaedic surgery (vs abdominal surgery) were not associated with increased odds of poor pain control. Study quality was generally high, although appropriate blinding of predictor during outcome ascertainment was often limited.
Conclusions: Nine predictors of poor postoperative pain control were identified. These should be recognised as potentially important factors when developing discipline-specific clinical care pathways to improve pain outcomes and to guide future surgical pain research.
Prospero registration number: CRD42017080682.
Keywords: meta-analysis; pain; pain scales; postoperative pain; preoperative predictors; surgery.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Total knee and hip replacement surgery projections show meteoric rise by 2030. Orthopaedic procedures set to continue gaining widespread acceptance as means to restore quality-of-life. Annual Meeting of the American Academy of Orthopaedic Surgery 2006.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases