

Addressing Profiles of Systemic Inflammation Across the Different Clinical Phenotypes of Acutely Decompensated Cirrhosis
- PMID: 30941129
- PMCID: PMC6434999
- DOI: 10.3389/fimmu.2019.00476
Addressing Profiles of Systemic Inflammation Across the Different Clinical Phenotypes of Acutely Decompensated Cirrhosis
Abstract
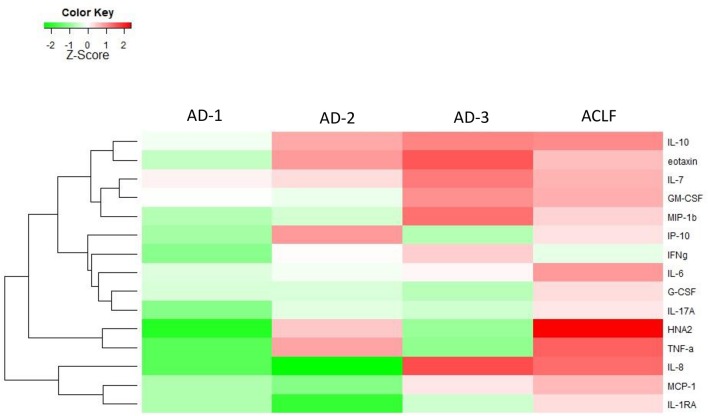
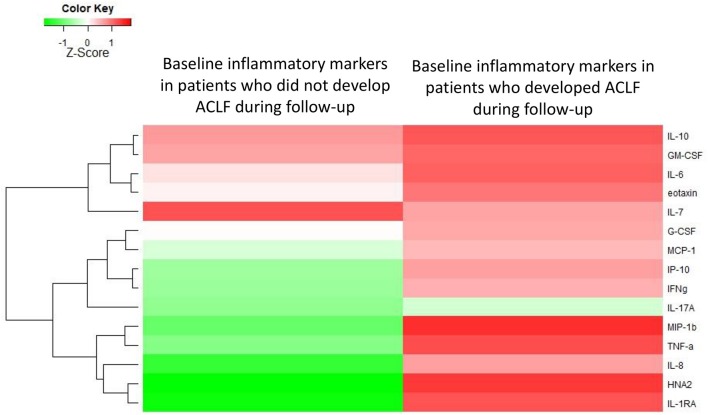
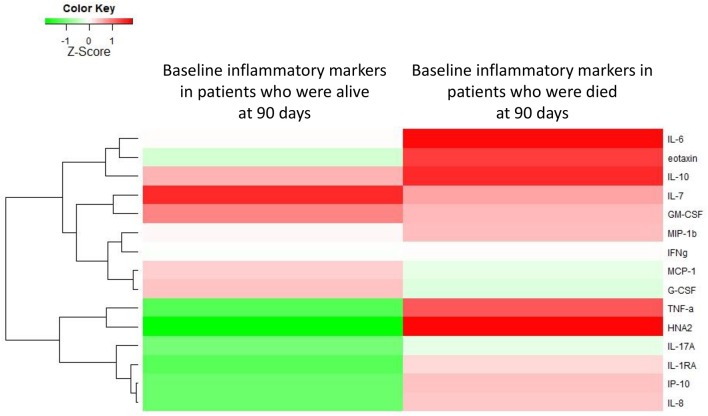
Background: Patients with acutely decompensated cirrhosis (AD) may or may not develop acute-on-chronic liver failure (ACLF). ACLF is characterized by high-grade systemic inflammation, organ failures (OF) and high short-term mortality. Although patients with AD cirrhosis exhibit distinct clinical phenotypes at baseline, they have low short-term mortality, unless ACLF develops during follow-up. Because little is known about the association of profile of systemic inflammation with clinical phenotypes of patients with AD cirrhosis, we aimed to investigate a battery of markers of systemic inflammation in these patients. Methods: Upon hospital admission baseline plasma levels of 15 markers (cytokines, chemokines, and oxidized albumin) were measured in 40 healthy controls, 39 compensated cirrhosis, 342 AD cirrhosis, and 161 ACLF. According to EASL-CLIF criteria, AD cirrhosis was divided into three distinct clinical phenotypes (AD-1: Creatinine<1.5, no HE, no OF; AD-2: creatinine 1.5-2, and or HE grade I/II, no OF; AD-3: Creatinine<1.5, no HE, non-renal OF). Results: Most markers were slightly abnormal in compensated cirrhosis, but markedly increased in AD. Patients with ACLF exhibited the largest number of abnormal markers, indicating "full-blown" systemic inflammation (all markers). AD-patients exhibited distinct systemic inflammation profiles across three different clinical phenotypes. In each phenotype, activation of systemic inflammation was only partial (30% of the markers). Mortality related to each clinical AD-phenotype was significantly lower than mortality associated with ACLF (p < 0.0001 by gray test). Among AD-patients baseline systemic inflammation (especially IL-8, IL-6, IL-1ra, HNA2 independently associated) was more intense in those who had poor 28-day outcomes (ACLF, death) than those who did not experience these outcomes. Conclusions: Although AD-patients exhibit distinct profiles of systemic inflammation depending on their clinical phenotypes, all these patients have only partial activation of systemic inflammation. However, those with the most extended baseline systemic inflammation had the highest the risk of ACLF development and death.
Keywords: ACLF; acute decompensation; cirrhosis; organ dysfunction; organ failure; signature.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials