

Tafenoquine and G6PD: a primer for clinicians
- PMID: 30941413
- PMCID: PMC6542331
- DOI: 10.1093/jtm/taz023
Tafenoquine and G6PD: a primer for clinicians
Abstract
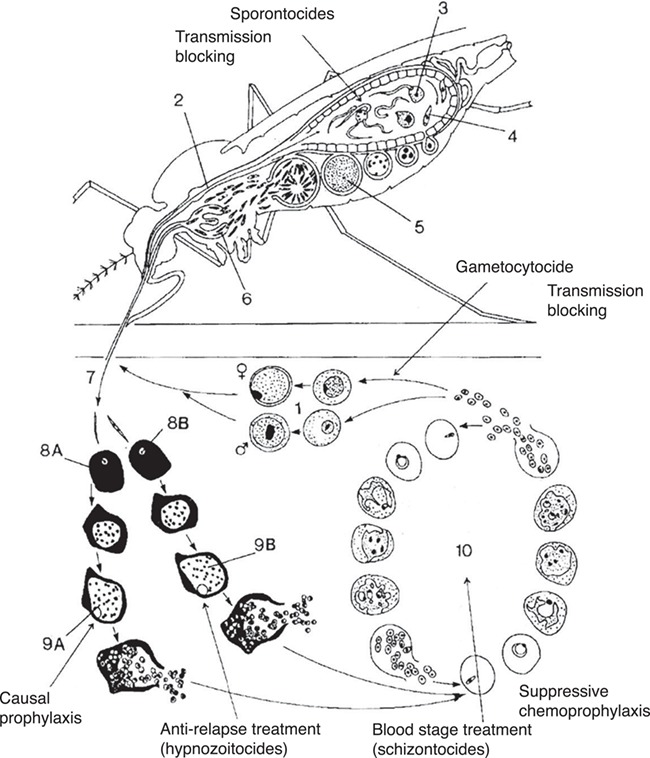
Background: Tafenoquine, an 8-aminoquinoline, is now indicated for causal prophylaxis against all human malarias and as radical curative (anti-relapse) treatment against Plasmodium vivax and Plasmodium ovale. As with other 8-aminoquinolines, tafenoquine causes hemolysis in individuals with glucose-6-phosphate dehydrogenase (G6PD) deficiency (hemizygous males and homozygous females) and is contraindicated in this population. Those with intermediate G6PD activity (heterozygous females) are also at risk for hemolysis. Awareness of how to prescribe tafenoquine in relation to G6PD status is needed so it can be used safely.
Methods: A standard literature search was performed on varying combinations of the terms tafenoquine, Arakoda, Kodatef, Krintafel, Kozenis, primaquine, G6PD deficiency, malaria prophylaxis and radical cure. The data were gathered and interpreted to review how tafenoquine should be prescribed in consideration of the G6PD status of an individual and traveller.
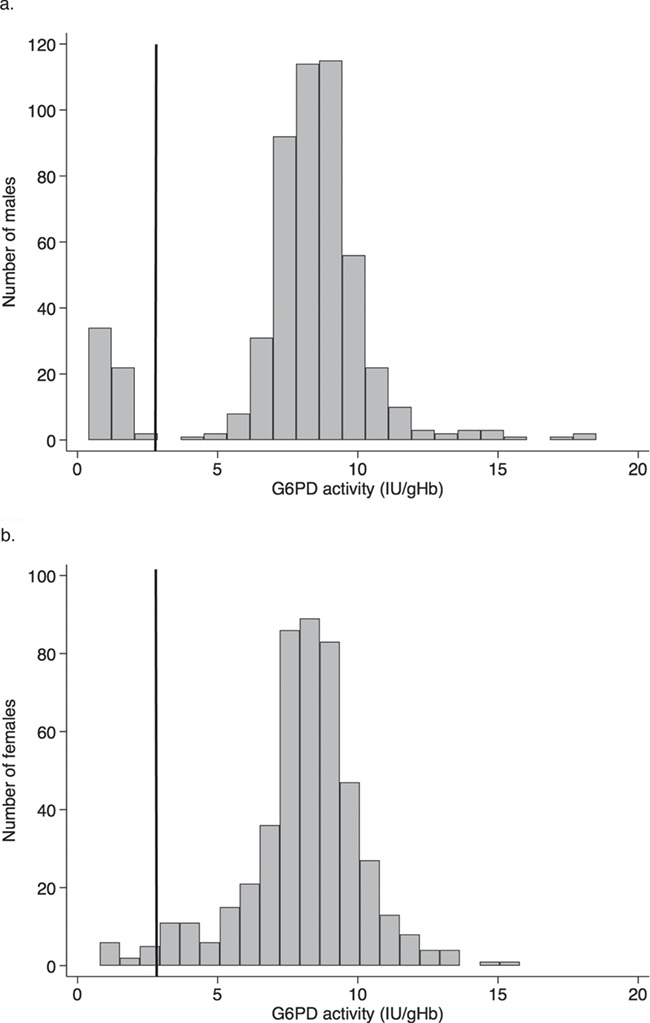
Results: Tafenoquine should only be given to those with G6PD activity >70% of the local population median. Qualitative G6PD tests are sufficient for diagnosing G6PD deficiency in males. However, in females quantitative G6PD testing is necessary to differentiate deficient, intermediate and normal G6PD statuses. Testing for G6PD deficiency is mandatory before tafenoquine prescription. Measures can be taken to avoid tafenoquine administration to ineligible individuals (i.e. due to G6PD status, age, pregnancy and lactation). Primaquine is still necessary for some of these cases. This review provides actions that can be taken to diagnose and manage hemolysis when tafenoquine is given inadvertently to ineligible individuals.
Conclusion: Attention to G6PD status is required for safe prescription of tafenoquine. A high index of suspicion is needed if hemolysis occurs. Clinicians should seek evidence-based information for the management and treatment of iatrogenicy hemolysis caused by 8-aminoquinolines.
Keywords: 8-aminoquinolines; causal prophylaxis; glucose-6-phosphate dehydrogenase deficiency; malaria prophylaxis; presumptive anti-relapse treatment (PART); radical cure; tafenoquine.
© International Society of Travel Medicine 2019. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
