

Association of Racial Disparities With Access to Kidney Transplant After the Implementation of the New Kidney Allocation System
- PMID: 30942882
- PMCID: PMC6583835
- DOI: 10.1001/jamasurg.2019.0512
Association of Racial Disparities With Access to Kidney Transplant After the Implementation of the New Kidney Allocation System
Abstract
Importance: Inactive patients on the kidney transplant wait-list have a higher mortality. The implications of this status change on transplant outcomes between racial/ethnic groups are unknown.
Objectives: To determine if activity status changes differ among races/ethnicities and levels of sensitization, and if these differences are associated with transplant probability after implementation of the Kidney Allocation System.
Design, setting, and participants: A multistate model was constructed from the Organ Procurement and Transplantation Network kidney transplant database (December 4, 2014, to September 8, 2016). The time interval followed Kidney Allocation System implementation and provided at least 1-year follow-up for all patients. The model calculated probabilities between active and inactive status and the following competing risk outcomes: living donor transplant, deceased donor transplant, and death/other. This retrospective cohort study included 42 558 patients on the Organ Procurement and Transplantation Network kidney transplant wait-list following Kidney Allocation System implementation. To rule out time-varying confounding from relisting, analysis was limited to first-time registrants. Owing to variations in listing practices, primary center listing data were used for dually listed patients. Individuals listed for another organ or pancreatic islets were excluded. Analysis began July 2017.
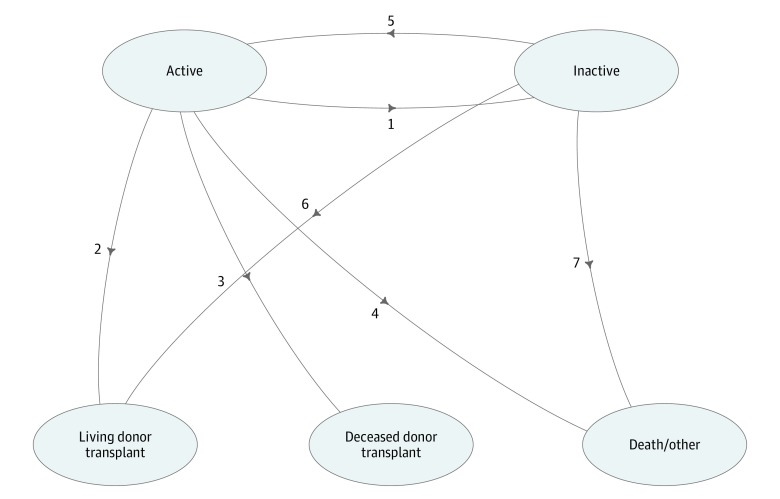
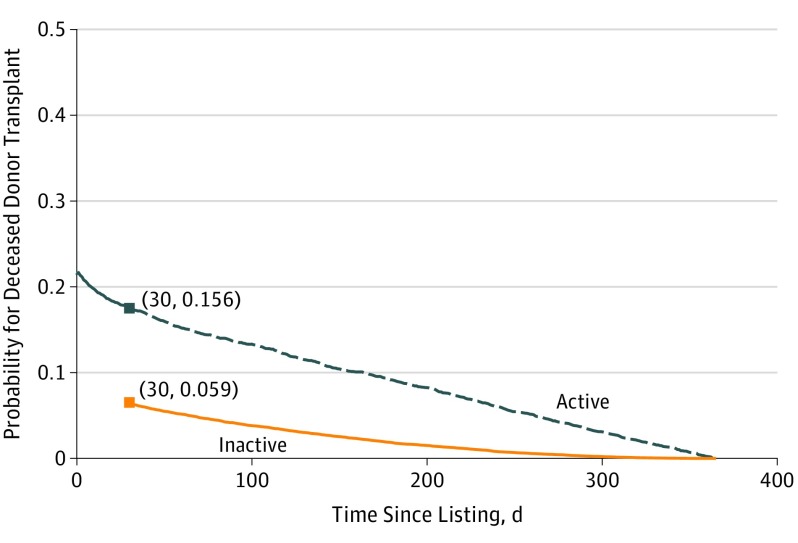
Main outcome and measures: Probabilities were determined for transitions between active and inactive status and the following outcome states: active to living donor transplant, active to deceased donor transplant, active to death/other, inactive to living donor transplant, inactive to deceased donor transplant, and inactive to death/other.
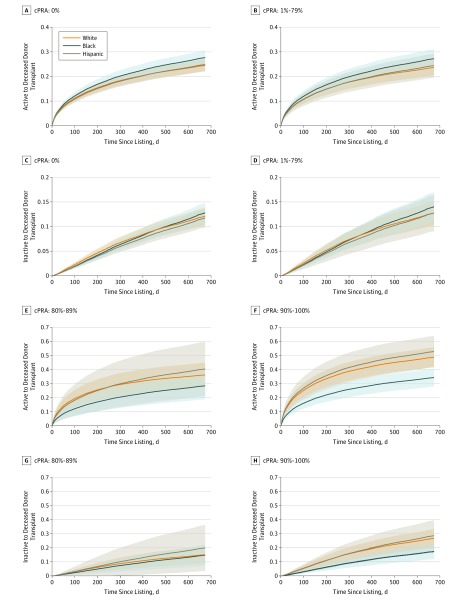
Results: The median (interquartile range) age at listing was 55.0 (18.0-89.0) years, and 26 535 of 42 558 (62.4%) were men. White individuals were 43.3% (n = 18 417) of wait-listed patients, while black and Hispanic individuals made up 27.8% (n = 11 837) and 19.5% (n = 8296), respectively. Patients in the calculated plasma reactive antibody categories of 0% or 1% to 79% showed no statistically significant difference in transplant probability among races/ethnicities. White individuals had an advantage in transplant probability over black individuals in calculated plasma reactive antibody categories of 80% to 89% (hazard ratio [HR], 1.8 [95% CI, 1.4-2.2]) and 90% or higher (HR, 2.4 [95% CI, 2.1-2.6]), while Hispanic individuals had an advantage over black individuals in the calculated plasma reactive antibody group of 90% or higher (HR, 2.5 [95% CI, 2.1-2.8]). Once on the inactive list, white individuals were more likely than Hispanic individuals (HR, 1.2 [95% CI, 1.17-1.3]) or black individuals (HR, 1.4 [95% CI, 1.3-1.4]) to resolve issues for inactivity resulting in activation.
Conclusions and relevance: For patients who are highly sensitized, there continues to be less access to kidney transplant in the black population after the implementation of the Kidney Allocation System. Health disparities continue after listing where individuals from minority groups have greater difficulty in resolving issues of inactivity.
Conflict of interest statement
Figures
Comment in
-
Barriers to Kidney Transplant-The Devil Is in the Details.JAMA Surg. 2019 Jul 1;154(7):625-626. doi: 10.1001/jamasurg.2019.0541. JAMA Surg. 2019. PMID: 30942876 No abstract available.
