

Percutaneous Endoscopic Decompression in Lumbar Canal and Lateral Recess Stenosis - The Surgical Learning Curve
- PMID: 30943708
- PMCID: PMC6449834
- DOI: 10.14245/ns.1938048.024
Percutaneous Endoscopic Decompression in Lumbar Canal and Lateral Recess Stenosis - The Surgical Learning Curve
Abstract
Objective: The purpose of this study is to characterize the learning curve of endoscopic lumbar decompression based on peri- and postoperative parameters and to suggest the potential of full endoscopic decompression as a primary treatment option for lumbar canal and lateral recess stenosis.
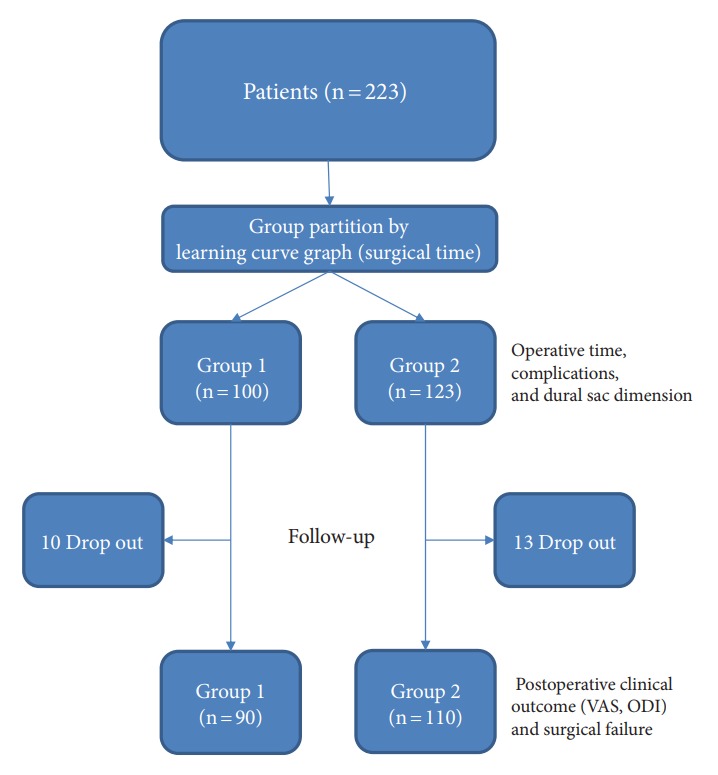
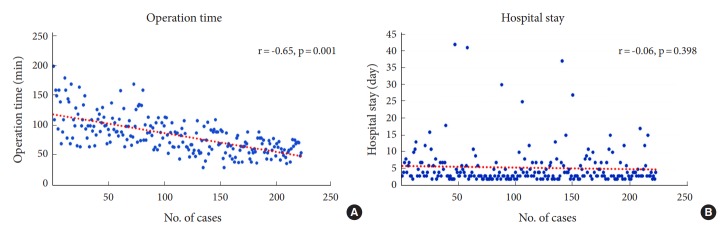
Methods: The records of 223 consecutive patients who underwent percutaneous endoscopic decompression by a single surgeon for their lumbar canal and lateral recess stenosis were reviewed. Patients were stratified into group 1 (n=100) and group 2 (n=123), depending on their case number. After the 100th case, the procedural time reached a plateau and subsequent patients were assigned to the second group. Demographics and surgical outcomes, including operative times, change in dural sac dimensions, length of hospital stay, and intraoperative complication rates were compared between the 2 groups. Postoperative clinical outcomes, including the visual analogue scale (VAS), the Oswestry Disability Index (ODI) and reoperation rates were compared between the 2 groups (group 1, n=90; group 2, n=110) by follow-up evaluation.
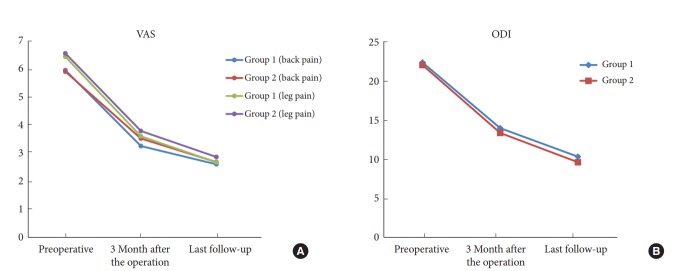
Results: Procedural times were greater in group 1 than group 2 (group 1, 105.26 minutes; group 2, 67.65 minutes; p<0.05) and they had higher complication rates (group 1, 16% [16 of 100]; group 2, 8.3% [8 of 123]; p<0.05). The length of hospitalization, postoperative improvement in VAS and ODI, and reoperation rates were not different between the groups. In both groups, stenotic spinal canals were effectively decompressed.
Conclusion: Continued surgical experience was associated with a reduction in operative times and less intraoperative complications. Although the learning curve was steep and additional surgical experience may be needed to overcome the learning curve, percutaneous full endoscopic lumbar decompression is a safe, clinically-feasible, and effective surgical technique and can be adopted as the primary treatment for lumbar canal and lateral recess stenosis.
Keywords: Learning curve; Lumbar canal decompression; Percutaneous endoscopic.
Conflict of interest statement
The authors have nothing to disclose.
Figures
References
-
- Kambin P, Brager MD. Percutaneous posterolateral discectomy. Anatomy and mechanism. Clin Orthop Relat Res. 1987;(223):145–54. - PubMed
-
- Yeung AT, Tsou PM. Posterolateral endoscopic excision for lumbar disc herniation: Surgical technique, outcome, and complications in 307 consecutive cases. Spine (Phila Pa 1976) 2002;27:722–31. - PubMed
-
- Hijikata S. Percutaneous nucleotomy. A new concept technique and 12 years' experience. Clin Orthop Relat Res. 1989;(238):9–23. - PubMed
-
- Phan K, Xu J, Schultz K, et al. Full-endoscopic versus microendoscopic and open discectomy: a systematic review and meta-analysis of outcomes and complications. Clin Neurol Neurosurg. 2017;154:1–12. - PubMed
-
- Akçakaya MO, Yörükoğlu AG, Aydoseli A, et al. Serum creatine phosphokinase levels as an indicator of muscle injury following lumbar disc surgery: comparison of fully endoscopic discectomy and microdiscectomy. Clin Neurol Neurosurg. 2016;145:74–8. - PubMed
LinkOut - more resources
Full Text Sources
