

Long-Term Outcomes Following Heart Team Revascularization Recommendations in Complex Coronary Artery Disease
- PMID: 30943827
- PMCID: PMC6507188
- DOI: 10.1161/JAHA.118.011279
Long-Term Outcomes Following Heart Team Revascularization Recommendations in Complex Coronary Artery Disease
Abstract
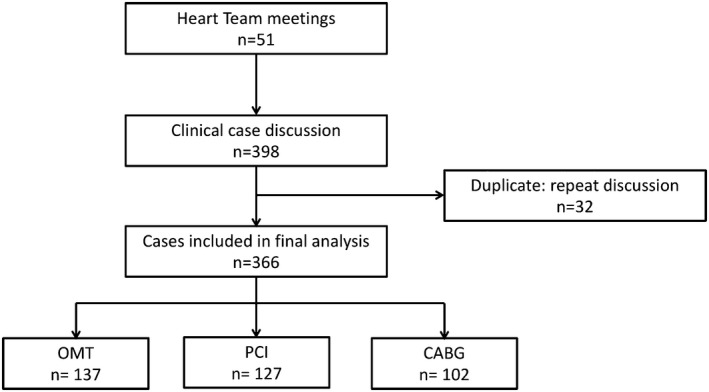
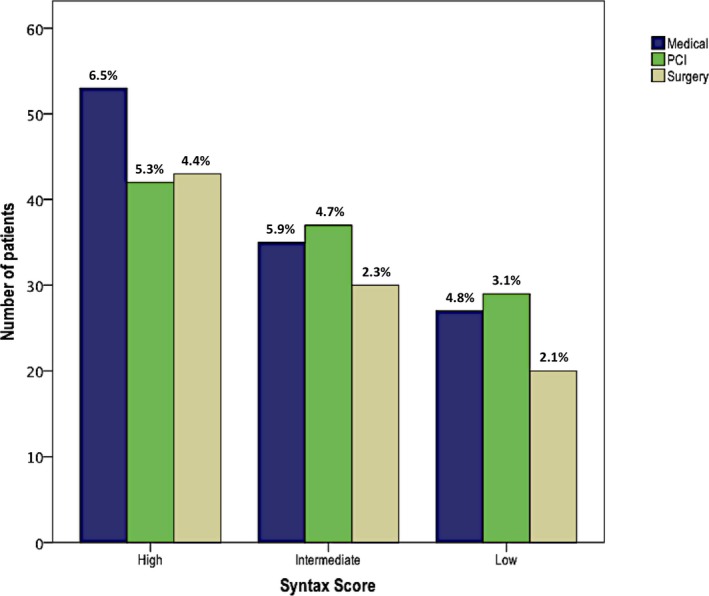
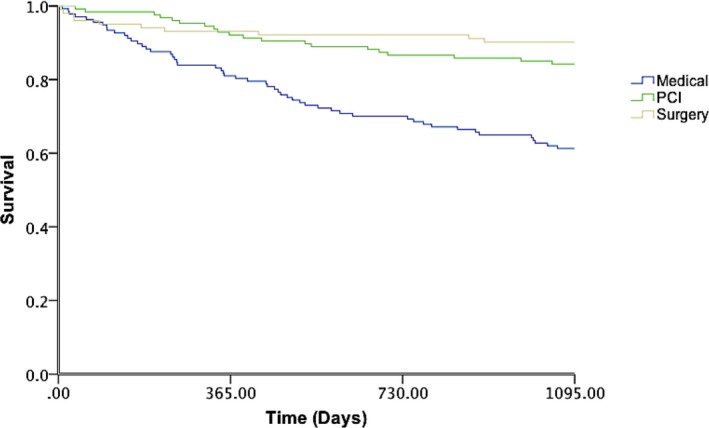
Background The Heart Team ( HT ) comprises integrated interdisciplinary decision making. Current guidelines assign a Class Ic recommendation for an HT approach to complex coronary artery disease ( CAD ). However, there remains a paucity of data in regard to hard clinical end points. The aim was to determine characteristics and outcomes in patients with complex CAD following HT discussion. Methods and Results This observational study was conducted at St Thomas' Hospital (London, UK). Case mixture included unprotected left main, 2-vessel (including proximal left anterior descending artery) CAD , 3-vessel CAD , or anatomical and/or clinical equipoise. HT strategy was defined as optimal medical therapy ( OMT ) alone, OMT +percutaneous coronary intervention ( PCI ), or OMT +coronary artery bypass grafting. From April 2012 to 2013, 51 HT meetings were held and 398 cases were discussed. Patients tended to have multivessel CAD (74.1%), high SYNTAX (Synergy between PCI with Taxus and Cardiac Surgery) scores (median, 30; interquartile range, 23-39), and average age 69±11 years. Multinomial logistic regression analysis performed to determine variables associated with HT strategy demonstrated decreased likelihood of undergoing PCI compared with OMT in older patients with chronic kidney disease and peripheral vascular disease. The odds of undergoing coronary artery bypass grafting compared with OMT decreased in the presence of cardiogenic shock and left ventricular dysfunction and increased in younger patients with 3-vessel CAD . Three-year survival was 60.8% (84 of 137) in the OMT cohort, 84.3% (107 of 127) in the OMT + PCI cohort, and 90.2% in the OMT +coronary artery bypass grafting cohort (92 of 102). Conclusions In our experience, the HT approach involved a careful selection process resulting in appropriate patient-specific decision making and good long-term outcomes in patients with complex CAD .
Keywords: Heart Team; coronary artery disease; health outcomes; medication therapy; revascularization.
Figures
References
-
- Blankenship JC, Gigliotti OS, Feldman DN, Mixon TA, Patel RAG, Sorajja P, Yakubov SJ, Chambers CE. Ad Hoc percutaneous coronary intervention: a consensus statement from the society for cardiovascular angiography and interventions. Catheter Cardiovasc Interv. 2012;81:748–758. - PubMed
-
- Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Nallamothu BK, Ting HH; American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines; Society for Cardiovascular Angiography and Interventions . 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58:e44–e122. - PubMed
-
- Serruys PW, Morice M‐C, Kappetein AP, Colombo A, Holmes DR, Mack MJ, Ståhle E, Feldman TE, van den Brand M, Bass EJ, Van Dyck N, Leadley K, Dawkins KD, Mohr FW; SYNTAX Investigators . Percutaneous coronary intervention versus coronary‐artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961–972. - PubMed
-
- Feit F, Brooks MM, Sopko G, Keller NM, Rosen A, Krone R, Berger PB, Shemin R, Attubato MJ, Williams DO, Frye R, Detre KM. Long‐term clinical outcome in the bypass angioplasty revascularization investigation registry. Circulation. 2000;101:2795–2802. - PubMed
-
- Nallamothu BK, Cohen DJ. No “i” in Heart Team: incentivizing multidisciplinary care in cardiovascular medicine. Circ Cardiovasc Qual Outcomes. 2012;5:410–413. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
