

Using country of origin to inform targeted tuberculosis screening in asylum seekers: a modelling study of screening data in a German federal state, 2002-2015
- PMID: 30943917
- PMCID: PMC6448304
- DOI: 10.1186/s12879-019-3902-x
Using country of origin to inform targeted tuberculosis screening in asylum seekers: a modelling study of screening data in a German federal state, 2002-2015
Abstract
Background: Screening programmes for tuberculosis (TB) among immigrants rarely consider the heterogeneity of risk related to migrants' country of origin. We assess the performance of a large screening programme in asylum seekers by analysing (i) the difference in yield and numbers needed to screen (NNS) by country and WHO-reported TB burden, (ii) the possible impact of screening thresholds on sensitivity, and (iii) the value of WHO-estimated TB burden to improve the prediction accuracy of screening yield.
Methods: We combined individual data of 119,037 asylum seekers screened for TB in Germany (2002-2015) with TB estimates of the World Health Organization (WHO) (1990-2014) for their 81 countries of origin. Adjusted rate ratios (aRR) and 95% credible intervals (CrI) of the observed yield of screening were calculated in Bayesian Poisson regression models by categories of WHO-estimated TB incidence. We assessed changes in sensitivity depending on screening thresholds, used WHO TB estimates as prior information to predict TB in asylum seekers, and modelled country-specific probabilities of numbers needed to screen (NNS) conditional on different screening thresholds.
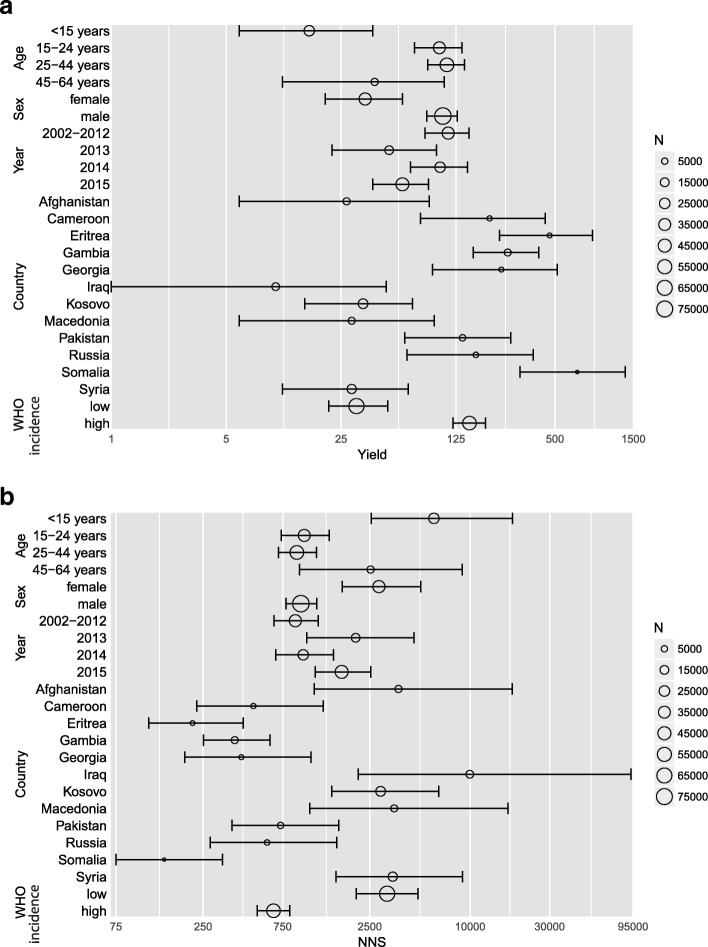
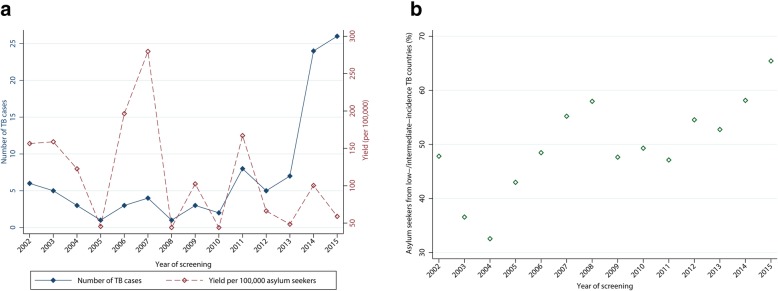
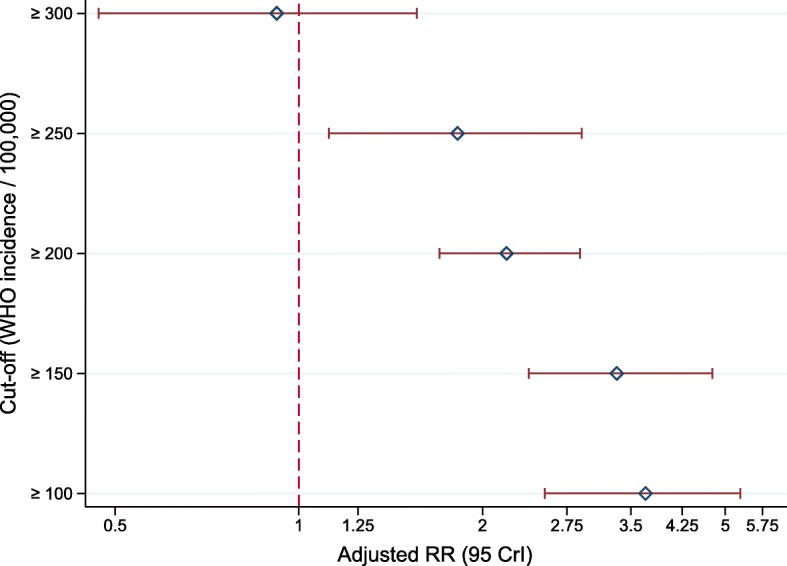
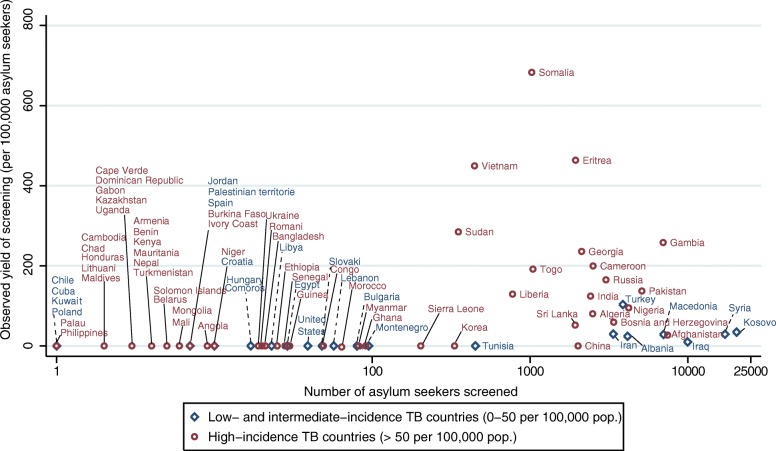
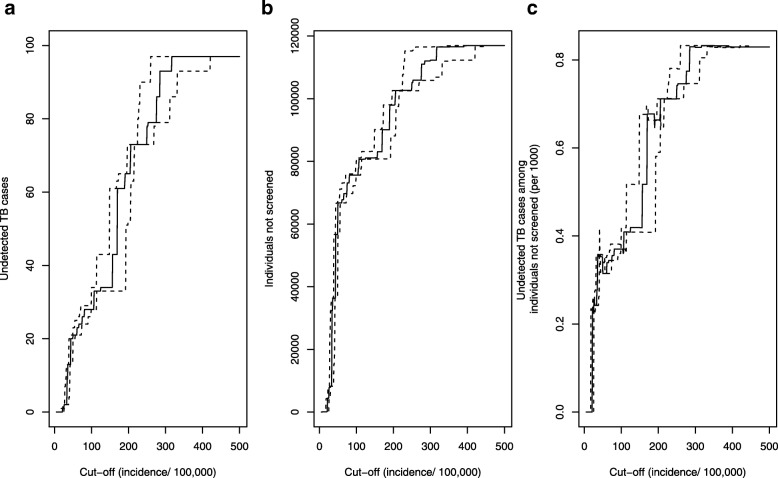
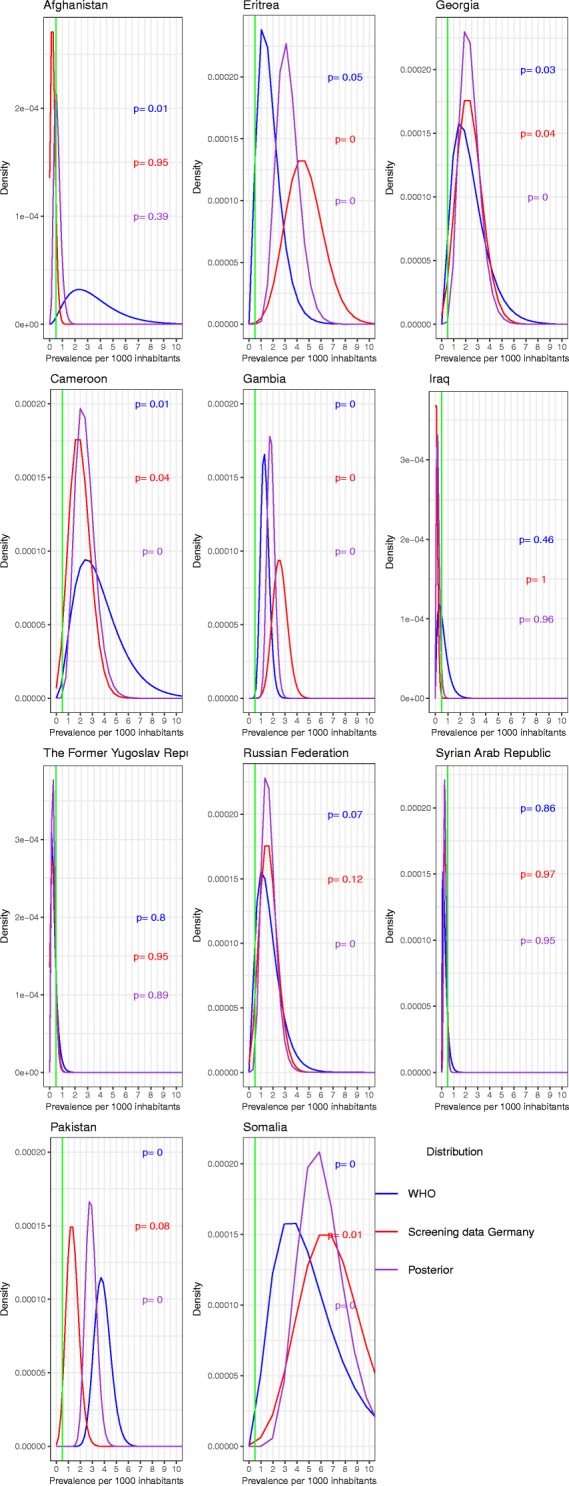
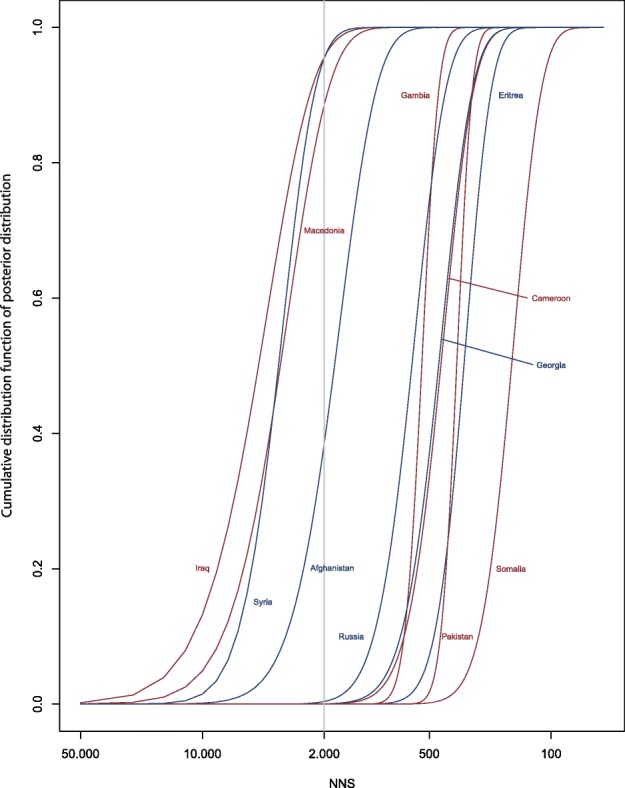
Results: The overall yield was 82 per 100,000 and the annual yield ranged from 44.1 to 279.7 per 100,000. Country-specific yields ranged from 10 (95%- CrI: 1-47) to 683 (95%-CrI: 306-1336) per 100,000 in Iraqi and Somali asylum seekers, respectively. The observed yield was higher in asylum seekers from countries with a WHO-estimated TB incidence > 50 relative to those from countries ≤50 per 100,000 (aRR: 4.17, 95%-CrI: 2.86-6.59). Introducing a threshold in the range of a WHO-estimated TB incidence of 50 and 100 per 100,000 resulted in the lowest "loss" in sensitivity. WHO's TB prevalence estimates improved prediction accuracy for eight of the 11 countries, and allowed modelling country-specific probabilities of NNS.
Conclusions: WHO's TB data can inform the estimation of screening yield and thus be used to improve screening efficiency in asylum seekers. This may help to develop more targeted screening strategies by reducing uncertainty in estimates of expected country-specific yield, and identify thresholds with lowest loss in sensitivity. Further modelling studies are needed which combine clinical, diagnostic and country-specific parameters.
Keywords: Asylum seekers; Efficiency; Epidemiology; Global health; Infection control; Migration; Modelling; Public health; Screening; Tuberculosis.
Conflict of interest statement
Ethics approval and consent to participate
The study findings are based on anonymous administrative data. This study is therefore exempt from ethical clearance according to the regulations of the Medical Ethics Committee of the Medical Faculty of Heidelberg University. Individual consent was not required due to the retrospective and anonymous nature of the study.
Consent for publication
The study findings are based on anonymous administrative data. Consent for publication is not required.
Competing interests
The material submitted in this manuscript is original and has not been submitted elsewhere. BJ was public health officer in the public health authority Karlsruhe until 2015. UW is public health officer in the public health authority Karlsruhe, Section for Disease Control, mandating the TB screening in the state reception centre Karlsruhe. CS is full time employee of Boehringer Ingelheim Pharma GmbH & Co. KG since October 2018. The company had no role in the design, analysis or interpretation of this study. Views expressed in this article are those of the authors and do not necessarily reflect those of Boehringer Ingelheim Pharma GmbH & Co. KG. The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Lönnroth K, Migliori GB, Abubakar I, D'Ambrosio L, de Vries G, Diel R, Douglas P, Falzon D, Gaudreau MA, Goletti D, González Ochoa ER, LoBue P, Matteelli A, Njoo H, Solovic I, Story A, Tayeb T, van der Werf MJ, Weil D, Zellweger JP, Abdel Aziz M, MRM AL, Aliberti S, de Onate WA, Barreira D, Bhatia V, Blasi F, Bloom A, Bruchfeld J, Castelli F, et al. Towards tuberculosis elimination: an action framework for low-incidence countries. Eur Respir J. 2015;45:928–952. doi: 10.1183/09031936.00214014. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
