

B-type natriuretic peptide trumps other prognostic markers in patients assessed for coronary disease
- PMID: 30943979
- PMCID: PMC6448253
- DOI: 10.1186/s12916-019-1306-9
B-type natriuretic peptide trumps other prognostic markers in patients assessed for coronary disease
Abstract
Background: Risk prediction for patients with suspected coronary artery disease is complex due to the common occurrence of prior cardiovascular disease and extensive risk modification in primary care. Numerous markers have the potential to predict prognosis and guide management, but we currently lack robust 'real-world' evidence for their use.
Methods: Prospective, multicentre observational study of consecutive patients referred for elective coronary angiography. Clinicians were blinded to all risk assessments, consisting of conventional factors, radial artery pulse wave analysis, 5-minute heart rate variability, high-sensitivity C-reactive protein and B-type natriuretic peptide (BNP). Blinded, independent adjudication was performed for all-cause mortality and the composite of death, myocardial infarction or stroke, analysed with Cox proportional hazards regression.
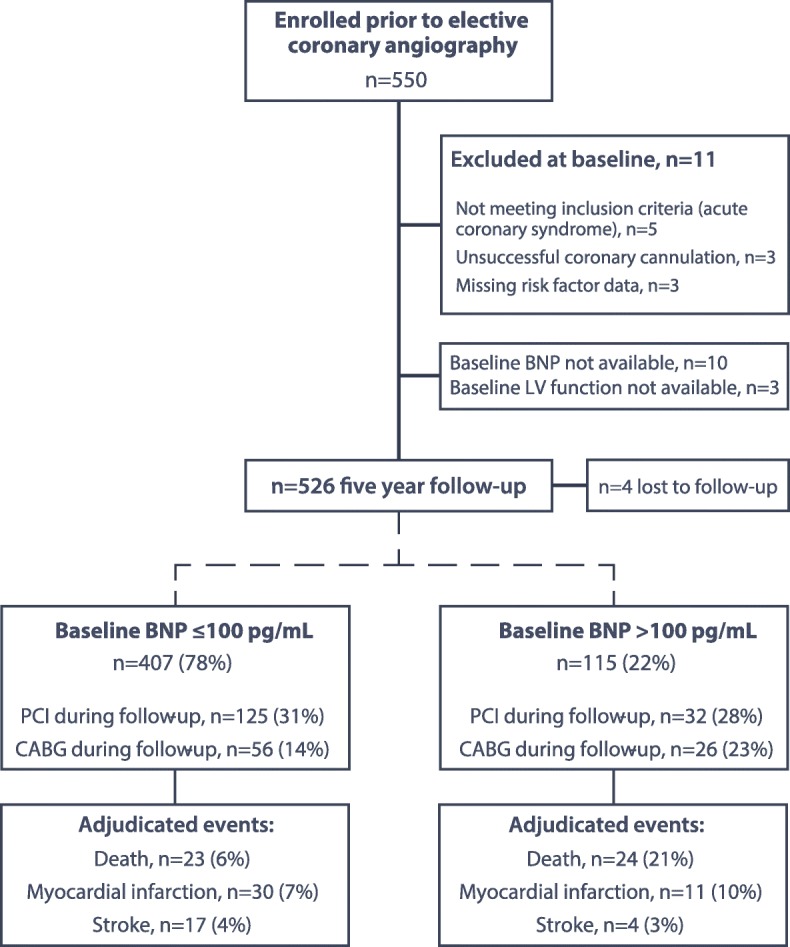
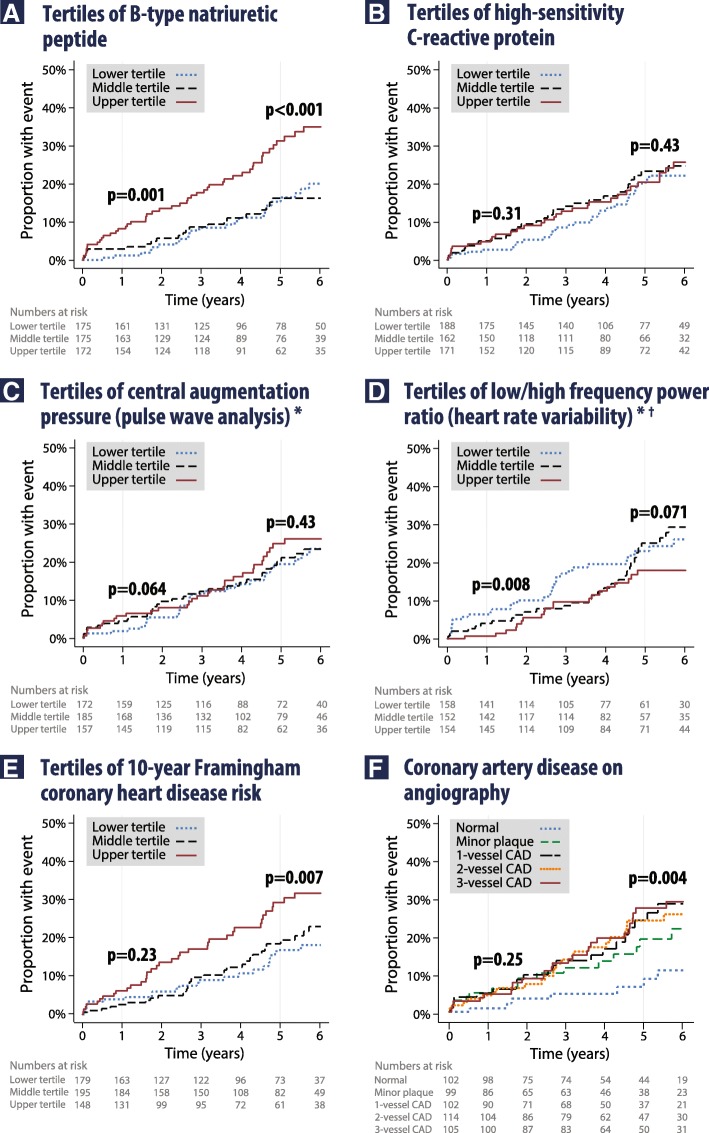
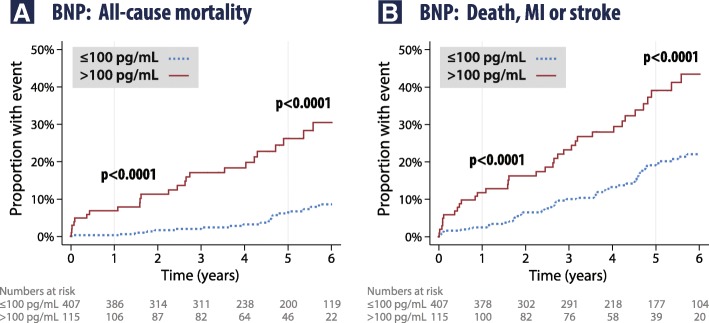
Results: Five hundred twenty-two patients were assessed with median age 66 years and 21% prior revascularization. Median baseline left ventricular ejection fraction was 64%, and 62% had ≥ 50% stenosis on angiography. During 5.0 years median follow-up, 30% underwent percutaneous and 16% surgical revascularization. In multivariate analysis, only age and BNP were independently associated with outcomes. The adjusted hazard ratio per log unit increase in BNP was 2.15 for mortality (95% CI 1.45-3.19; p = 0.0001) and 1.27 for composite events (1.04-1.54; p = 0.018). Patients with baseline BNP > 100 pg/mL had substantially higher mortality and composite events (20.9% and 32.2%) than those with BNP ≤ 100 pg/mL (5.6% and 15.5%). BNP improved both classification and discrimination of outcomes (p ≤ 0.003), regardless of left ventricular systolic function. Conversely, high-sensitivity C-reactive protein, pulse wave analysis and heart rate variability were unrelated to prognosis at 5 years after risk modification and treatment of coronary disease.
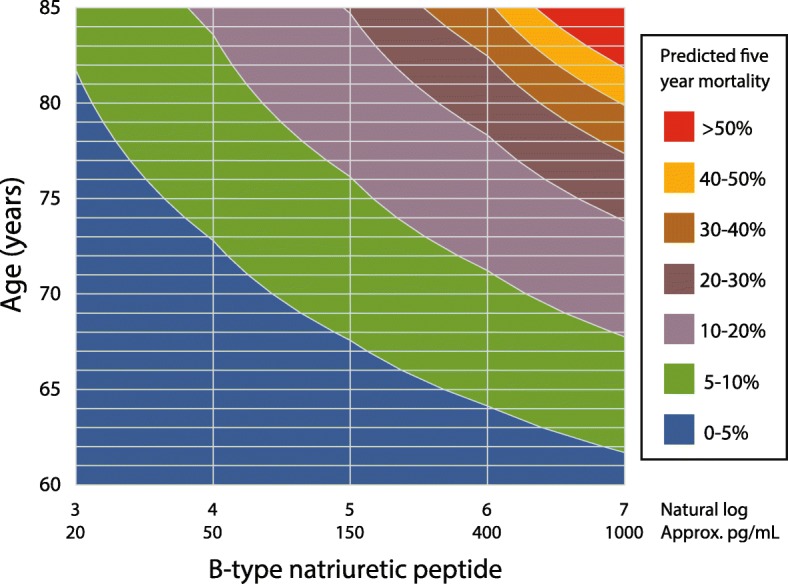
Conclusions: Conventional risk factors and other markers of arterial compliance, inflammation and autonomic function have limited value for prediction of outcomes in risk-modified patients assessed for coronary disease. BNP can independently identify patients with subtle impairment of cardiac function that might benefit from more intensive management.
Trial registration: Clinicaltrials.gov, NCT00403351 Registered on 22 November 2006.
Keywords: B-type natriuretic peptide; Coronary angiography; Coronary artery disease; Mortality; Risk.
Conflict of interest statement
Ethics approval and consent to participate
The ARM-CAD Study was approved by Ethics Committees from Monash University, Melbourne, Australia (2006/831MC) and The Alfred Melbourne, Australia (38/07).
All patients provided written informed consent.
Consent for publication
Not applicable – all original data.
Competing interests
MDF reports grants from Novartis and personal fees from AstraZeneca, Novartis and Pfizer, all outside the submitted work. DA has received speakers’ honoraria from Roche Diagnostics and Siemens Diagnostics, outside the submitted work. PC reports personal speaking honoraria from Menarini, AstraZenica, Bayer, Itamar Medical, Abbott and Ferring Pharmaceuticals, all outside the submitted work. The other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bottle A, Mozid A, Grocott HP, Walters MR, Lees KR, Aylin P, et al. Preoperative risk factors in 10 418 patients with prior myocardial infarction and 5241 patients with prior unstable angina undergoing elective coronary artery bypass graft surgery. Br J Anaesth. 2013;111:417–423. doi: 10.1093/bja/aet107. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
