An individualised versus a conventional pneumoperitoneum pressure strategy during colorectal laparoscopic surgery: rationale and study protocol for a multicentre randomised clinical study
- PMID: 30944044
- PMCID: PMC6446296
- DOI: 10.1186/s13063-019-3255-1
An individualised versus a conventional pneumoperitoneum pressure strategy during colorectal laparoscopic surgery: rationale and study protocol for a multicentre randomised clinical study
Erratum in
-
Correction to: An individualised versus a conventional pneumoperitoneum pressure strategy during colorectal laparoscopic surgery: rationale and study protocol for a multicentre randomised clinical study.Trials. 2020 Jan 13;21(1):70. doi: 10.1186/s13063-020-4055-3. Trials. 2020. PMID: 31931888 Free PMC article.
Abstract
Background: A recent study shows that a multifaceted strategy using an individualised intra-abdominal pressure titration strategy during colorectal laparoscopic surgery results in an acceptable workspace at low intra-abdominal pressure in most patients. The multifaceted strategy, focused on lower to individualised intra-abdominal pressures, includes prestretching the abdominal wall during initial insufflation, deep neuromuscular blockade, low tidal volume ventilation settings and a modified lithotomy position. The study presented here tests the hypothesis that this strategy improves outcomes of patients scheduled for colorectal laparoscopic surgery.
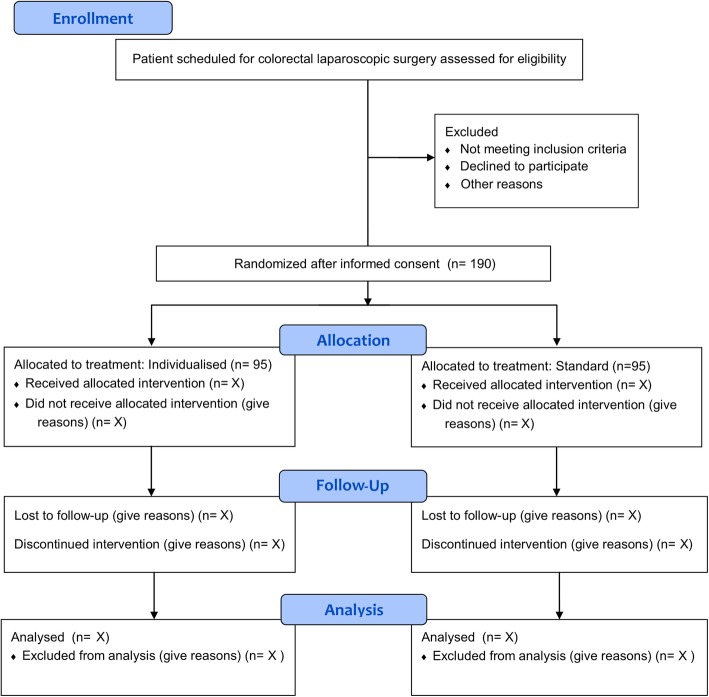
Methods: The Individualized Pneumoperitoneum Pressure in Colorectal Laparoscopic Surgery versus Standard Therapy (IPPCollapse-II) study is a multicentre, two-arm, parallel-group, single-blinded randomised 1:1 clinical study that runs in four academic hospitals in Spain. Patients scheduled for colorectal laparoscopic surgery with American Society of Anesthesiologists classification I to III who are aged > 18 years and are without cognitive deficits are randomised to an individualised pneumoperitoneum pressure strategy (the intervention group) or to a conventional pneumoperitoneum pressure strategy (the control group). The primary outcome is recovery assessed with the Post-operative Quality of Recovery Scale (PQRS) at postoperative day 1. Secondary outcomes include PQRS score in the post anaesthesia care unit and at postoperative day 3, postoperative complications until postoperative day 28, hospital length of stay and process-related outcomes.
Discussion: The IPPCollapse-II study will be the first randomised clinical study that assesses the impact of an individualised pneumoperitoneum pressure strategy focused on working with the lowest intra-abdominal pressure during colorectal laparoscopic surgery on relevant patient-centred outcomes. The results of this large study, to be disseminated through conference presentations and publications in international peer-reviewed journals, are of ultimate importance for optimising the care and safety of laparoscopic abdominal surgery. Selection of patient-reported outcomes as the primary outcome of this study facilitates the translation into clinical practice. Access to source data will be made available through anonymised datasets upon request and after agreement of the Steering Committee of the IPPCollapse-II study.
Trial registration: ClinicalTrials.gov, NCT02773173 . Registered on 16 May 2016. EudraCT, 2016-001693-15. Registered on 8 August 2016.
Keywords: Abdominal laparoscopy; Colorectal surgery; Outcome; Pneumoperitoneum pressure; Post-operative Quality of Recovery Scale (PQRS); Postoperative complications; Safety.
Conflict of interest statement
Ethics approval and consent to participate
The study will be carried out according to a protocol reviewed and approved at a national level by the Institutional Review Board (IRB) of Hospital Universitari i Politècnic La Fe, Valencia, Spain, and Agencia Española del Medicamento y Productos Sanitarios (AEMPS). The study has been registered at ClinicalTrials.gov (identifier NCT02773173, May 16, 2016) and EudraCT (2016-001693-15), and is conducted in accordance with the Declaration of Helsinki on ethical principles for medical research in human subjects, adopted by the General Assembly of the World Medical Association (1996). Data management, monitoring and reporting of the study are performed in accordance with the International Conference on Harmonisation Good Clinical Practice guidelines (ICH) (CPMP/ICH/135/95) and the regulatory requirements for participating institutions by the Spanish Clinical Research Network (SCReN). Investigators collect a written informed consent form in compliance with the GCP recommendations to the patient or his/her legal representative if the patient’s clinical conditions do not allow him/her to review and approve it. Investigators provide a copy of the signed informed consent form to each subject and keep a copy in the subject’s study file.
Consent for publication
Not applicable.
Competing interests
Oscar Diaz-Cambronero received a grant from the Merck Investigator Studies Program Review Committee (MISP-RC), Merck Sharp & Dohme, protocol code #53607 with $109,672 and speakers’ fees and honoraria from Merck Sharp & Dohme for lectures (€8.000); Carlos L. Errando received speakers’ fees and honoraria for lectures from Merck Sharp & Dohme (€1.000); Blas Flor Lorente received speakers’ fees and honoraria from Merck Sharp & Dohme for lectures (€3.000); Maria Pilar Argente Navarro received speakers’ fees and honoraria for lectures from Merck Sharp & Dohme (€1.000); Guido Mazzinari, Nuria Garcia Gregorio, Maria Vila Montañes, Daniel Robles Hernandez, Luis Enrique Olmedilla Arnal, Angel Martín de Pablos, Anabel Marques Marí and Marcus J. Schultz declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures