

Prevalence of cervical disease at age 20 after immunisation with bivalent HPV vaccine at age 12-13 in Scotland: retrospective population study
- PMID: 30944092
- PMCID: PMC6446188
- DOI: 10.1136/bmj.l1161
Prevalence of cervical disease at age 20 after immunisation with bivalent HPV vaccine at age 12-13 in Scotland: retrospective population study
Abstract
Objective: To quantify the effect on cervical disease at age 20 years of immunisation with bivalent human papillomavirus (HPV) vaccine at age 12-13 years.
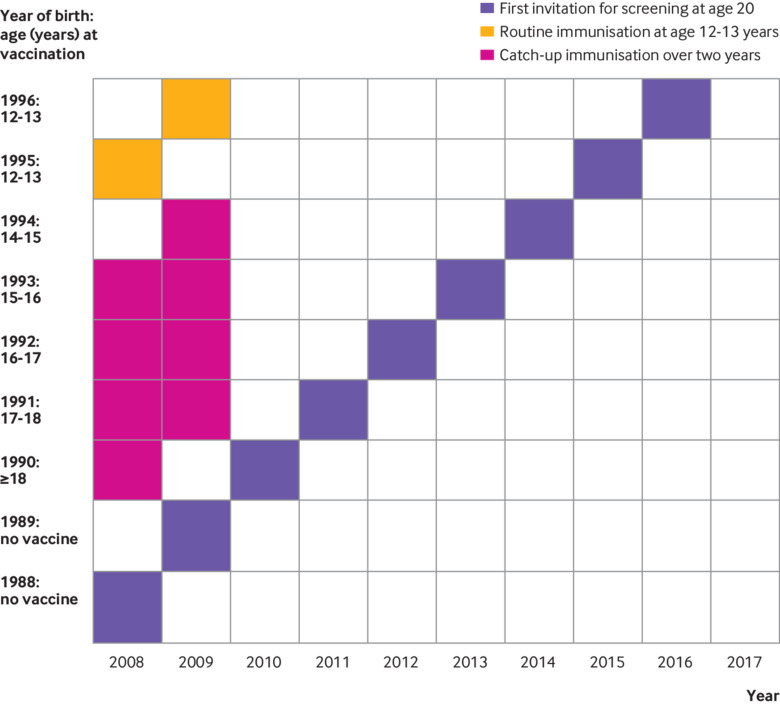
Design: Retrospective population study, 1988-96.
Setting: National vaccination and cervical screening programmes in Scotland.
Participants: 138 692 women born between 1 January 1988 and 5 June 1996 and who had a smear test result recorded at age 20.
Main outcome measures: Effect of vaccination on cytology results and associated histological diagnoses from first year of screening (while aged 20), calculated using logistic regression.
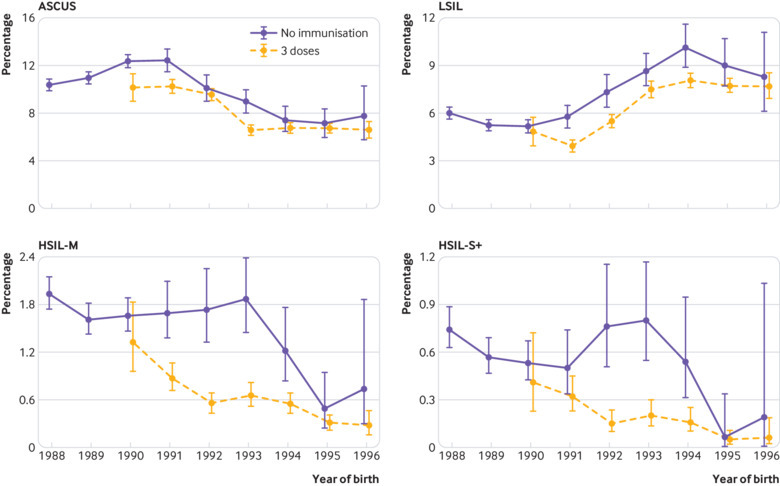
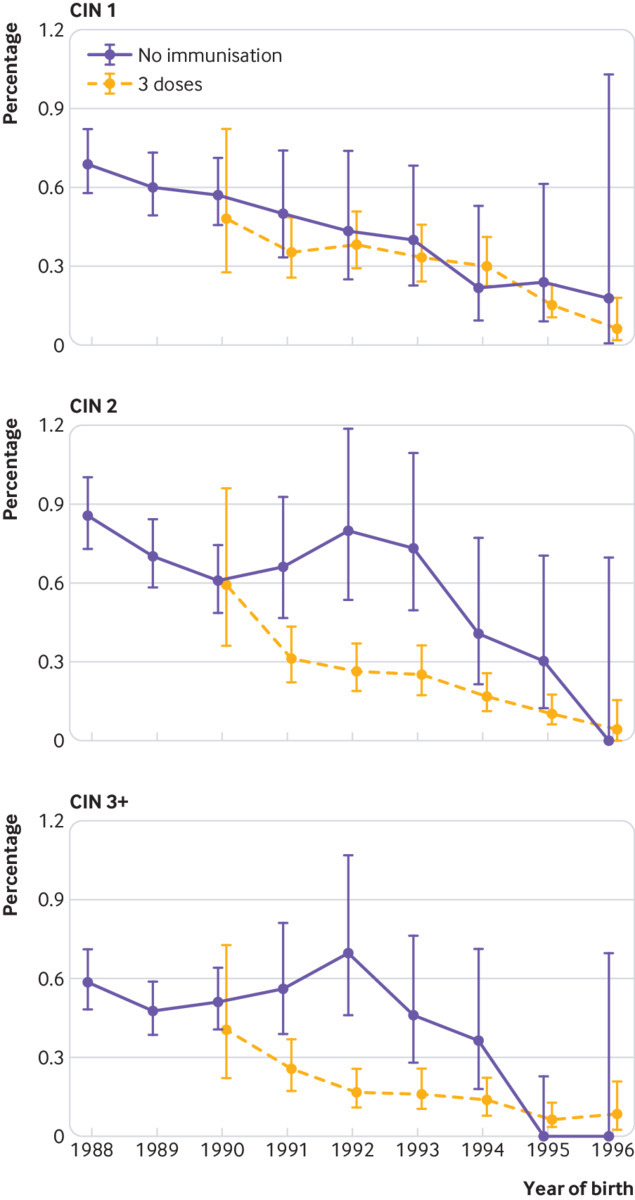
Results: 138 692 records were retrieved. Compared with unvaccinated women born in 1988, vaccinated women born in 1995 and 1996 showed an 89% reduction (95% confidence interval 81% to 94%) in prevalent cervical intraepithelial neoplasia (CIN) grade 3 or worse (from 0.59% (0.48% to 0.71%) to 0.06% (0.04% to 0.11%)), an 88% reduction (83% to 92%) in CIN grade 2 or worse (from 1.44% (1.28% to 1.63%) to 0.17% (0.12% to 0.24%)), and a 79% reduction (69% to 86%) in CIN grade 1 (from 0.69% (0.58% to 0.63%) to 0.15% (0.10% to 0.21%)). Younger age at immunisation was associated with increasing vaccine effectiveness: 86% (75% to 92%) for CIN grade 3 or worse for women vaccinated at age 12-13 compared with 51% (28% to 66%) for women vaccinated at age 17. Evidence of herd protection against high grade cervical disease was found in unvaccinated girls in the 1995 and 1996 cohorts.
Conclusions: Routine vaccination of girls aged 12-13 years with the bivalent HPV vaccine in Scotland has led to a dramatic reduction in preinvasive cervical disease. Evidence of clinically relevant herd protection is apparent in unvaccinated women. These data are consistent with the reduced prevalence of high risk HPV in Scotland. The bivalent vaccine is confirmed as being highly effective vaccine and should greatly reduce the incidence of cervical cancer. The findings will need to be considered by cervical cancer prevention programmes worldwide.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: KP has received travel monies from both Merck and GSK to attend conferences. KC’s institution has received monies to deliver research, or associated consumables to support research, from: Qiagen, Hologic, Selfscreen, GeneFirst, Euroimmun, Cepheid, Genomica, and LifeRiver. No personal conflicts of interest are declared.
Figures
Comment in
-
The remarkable impact of bivalent HPV vaccine in Scotland.BMJ. 2019 Apr 3;365:l1375. doi: 10.1136/bmj.l1375. BMJ. 2019. PMID: 30944088 No abstract available.
References
-
- GLOBOCAN Cervical cancer fact sheet. http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx.
-
- Cancer Research UK www.cancerresearchuk.org/health-professional/cancer-statistics/statistic....
-
- Information Services Division. Scotland. Estimate of HPV vaccine uptake in Scotland, by year of birth. https://isdscotland.scot.nhs.uk/Health-Topics/Child-Health/publications/....
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical