

Large-scale plasma metabolome analysis reveals alterations in HDL metabolism in migraine
- PMID: 30944236
- PMCID: PMC6550500
- DOI: 10.1212/WNL.0000000000007313
Large-scale plasma metabolome analysis reveals alterations in HDL metabolism in migraine
Abstract
Objective: To identify a plasma metabolomic biomarker signature for migraine.
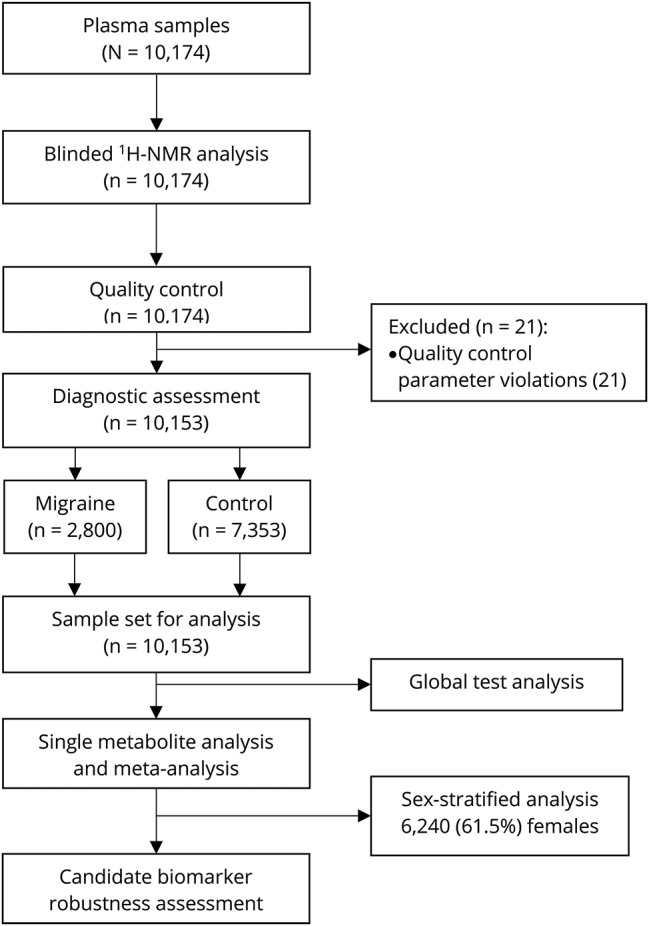
Methods: Plasma samples from 8 Dutch cohorts (n = 10,153: 2,800 migraine patients and 7,353 controls) were profiled on a 1H-NMR-based metabolomics platform, to quantify 146 individual metabolites (e.g., lipids, fatty acids, and lipoproteins) and 79 metabolite ratios. Metabolite measures associated with migraine were obtained after single-metabolite logistic regression combined with a random-effects meta-analysis performed in a nonstratified and sex-stratified manner. Next, a global test analysis was performed to identify sets of related metabolites associated with migraine. The Holm procedure was applied to control the family-wise error rate at 5% in single-metabolite and global test analyses.
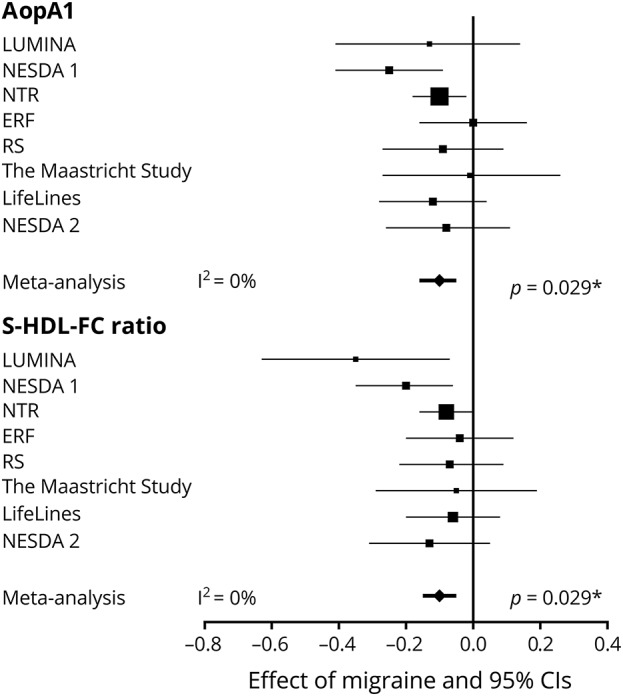
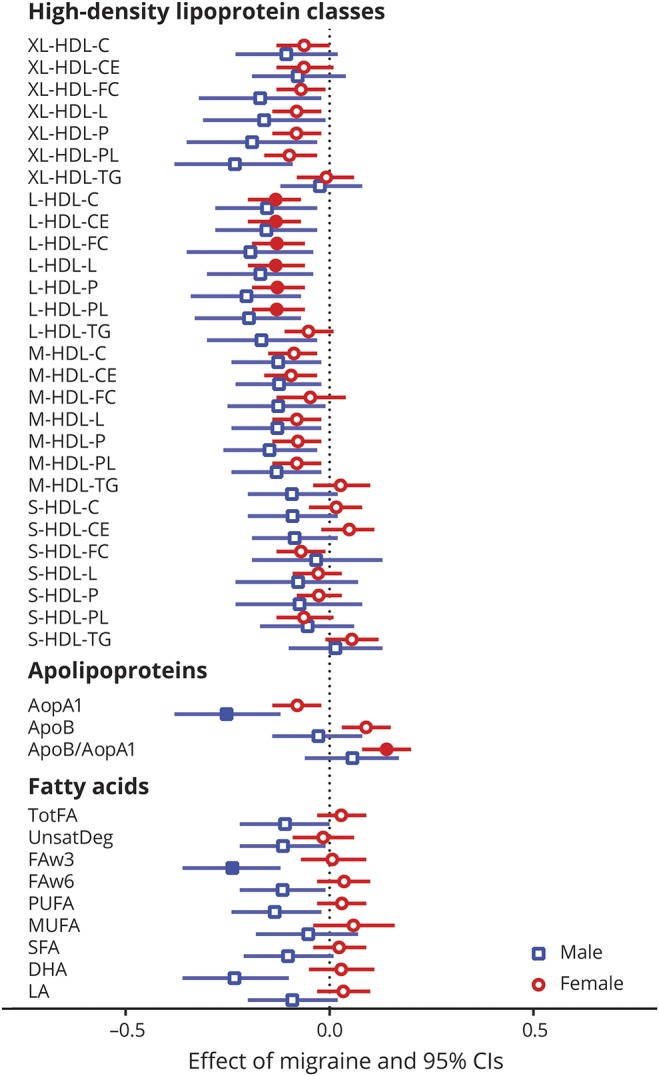
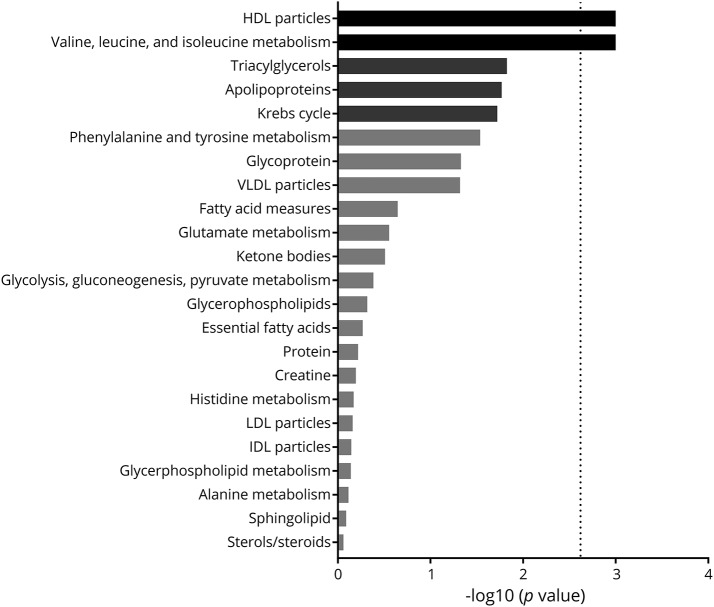
Results: Decreases in the level of apolipoprotein A1 (β -0.10; 95% confidence interval [CI] -0.16, -0.05; adjusted p = 0.029) and free cholesterol to total lipid ratio present in small high-density lipoprotein subspecies (HDL) (β -0.10; 95% CI -0.15, -0.05; adjusted p = 0.029) were associated with migraine status. In addition, only in male participants, a decreased level of omega-3 fatty acids (β -0.24; 95% CI -0.36, -0.12; adjusted p = 0.033) was associated with migraine. Global test analysis further supported that HDL traits (but not other lipoproteins) were associated with migraine status.
Conclusions: Metabolic profiling of plasma yielded alterations in HDL metabolism in migraine patients and decreased omega-3 fatty acids only in male migraineurs.
Copyright © 2019 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
Metabolite profiling links lipids to migraine.Nat Rev Neurol. 2019 Jun;15(6):308. doi: 10.1038/s41582-019-0192-2. Nat Rev Neurol. 2019. PMID: 31015642 No abstract available.
References
-
- Launer LJ, Terwindt GM, Ferrari MD. The prevalence and characteristics of migraine in a population-based cohort: the GEM study. Neurology 1999;53:537–542. - PubMed
-
- Stovner LJ, Zwart JA, Hagen K, Terwindt GM, Pascual J. Epidemiology of headache in Europe. Eur J Neurol 2006;13:333–345. - PubMed
-
- Jensen R, Stovner LJ. Epidemiology and comorbidity of headache. Lancet Neurol 2008;7:354–361. - PubMed
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017;390:1211–1259. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical