

Outcomes with ambulatory advanced heart failure from the Medical Arm of Mechanically Assisted Circulatory Support (MedaMACS) Registry
- PMID: 30948210
- PMCID: PMC6452871
- DOI: 10.1016/j.healun.2018.09.021
Outcomes with ambulatory advanced heart failure from the Medical Arm of Mechanically Assisted Circulatory Support (MedaMACS) Registry
Abstract
Background: The outlook for ambulatory patients with advanced heart failure (HF) and the appropriate timing for left ventricular assist device (LVAD) or transplant remain uncertain. The aim of this study was to better understand disease trajectory and rates of progression to subsequent LVAD therapy and transplant in ambulatory advanced HF.
Methods: Patients with advanced HF who were New York Heart Association (NYHA) Class III or IV and Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) Profiles 4 to 7, despite optimal medical therapy (without inotropic therapy), were enrolled across 11 centers and followed for the end-points of survival, transplantation, LVAD placement, and health-related quality of life. A secondary intention-to-treat survival analysis compared outcomes for MedaMACS patients with a matched group of Profile 4 to 7 patients with LVADs from the INTERMACS registry.
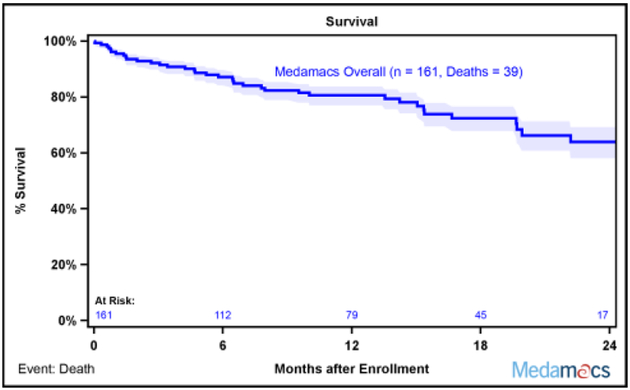
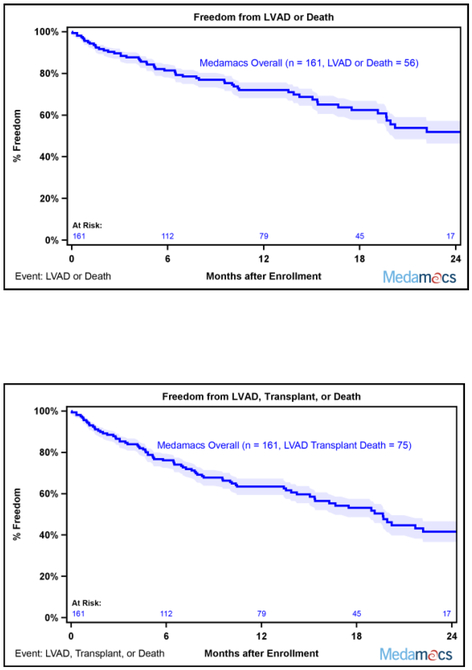
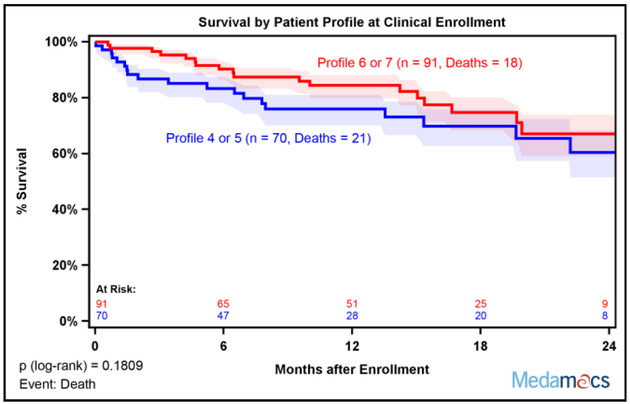
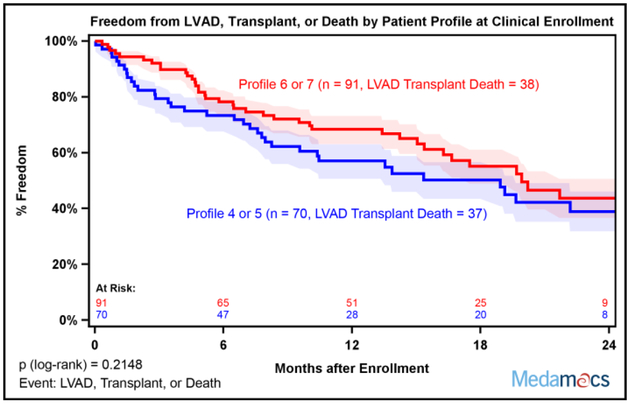
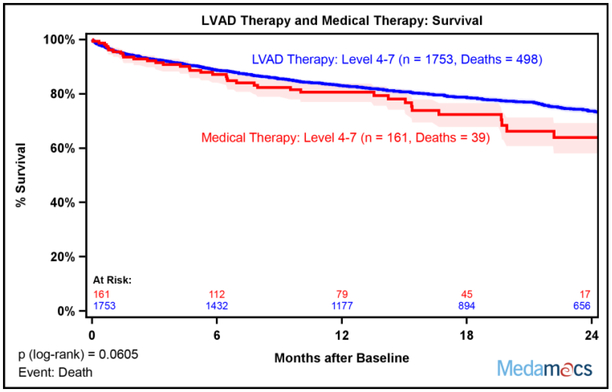
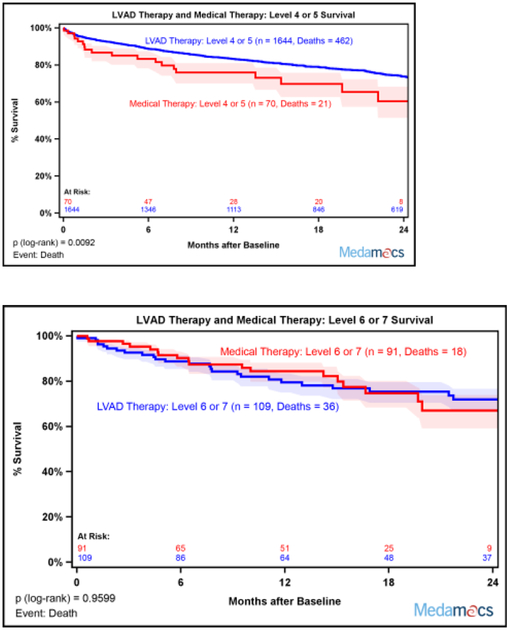
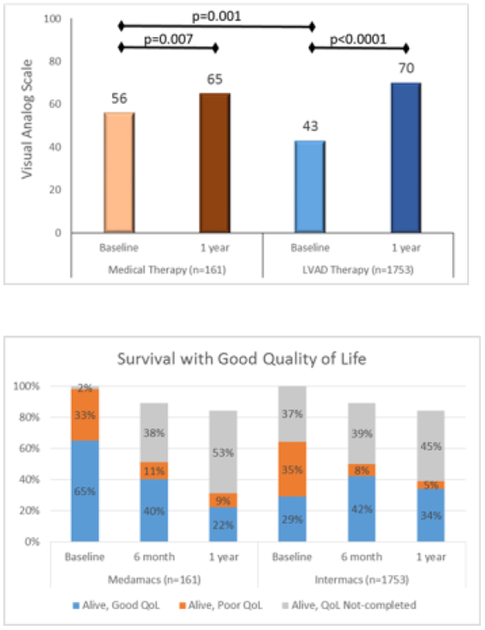
Results: Between May 2013 and October 2015, 161 patients were enrolled with INTERMACS Profiles 4 (12%), 5 (32%), 6 (49%), and 7 (7%). By 2 years after enrollment, 75 (47%) patients had reached a primary end-point with 39 (24%) deaths, 17 (11%) undergoing LVAD implantation, and 19 (12%) receiving a transplant. Compared with 1,753 patients with Profiles 4 to 7 receiving LVAD therapy, there was no overall difference in intention-to-treat survival between medical and LVAD therapy, but survival with LVAD therapy was superior to medical therapy among Profile 4 and 5 patients (p = 0.0092). Baseline health-related quality of life was lower among patients receiving a LVAD than those enrolled on continuing oral medical therapy, but increased after 1 year for survivors in both cohorts.
Conclusions: Ambulatory patients with advanced HF are at high risk for poor outcomes, with only 53% alive on medical therapy after 2 years of follow-up. Survival was similar for medical and LVAD therapy in the overall cohort, which included the lower severity Profiles 6 and 7, but survival was better with LVAD therapy among patients in Profiles 4 and 5. Given the poor outcomes in this group of advanced HF patients, timely consideration of transplant and LVAD is of critical importance.
Keywords: advanced heart failure; cardiac transplantation; mechanical circulatory support; patient decision-making; ventricular assist device.
Copyright © 2018 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Disclosures
Dr. DeVore reports receiving research support from the American Heart Association, Amgen, the NIH, and Novartis and consulting with Novartis. Dr. Teuteberg reports receiving advertising board and speaking honoraria from Medtronic, CareDx, and Abiomed as well as receiving support from Abbott for the HeartMate 3 Clinical Events Committee. The remaining authors have no disclosures.
Figures
Comment in
-
Timing of mechanically assisted circulatory support.J Heart Lung Transplant. 2019 Apr;38(4):418-419. doi: 10.1016/j.healun.2019.01.1308. Epub 2019 Jan 29. J Heart Lung Transplant. 2019. PMID: 30770267 No abstract available.
References
-
- Kirklin JK, Pagani FD, Kormos RL, et al. Eighth annual INTERMACS report: Special focus on framing the impact of adverse events. J Heart Lung Transplant 2017;36:1080–6. - PubMed
-
- Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med 2001;345:1435–43. - PubMed
-
- Hashim T, Sanam K, Revilla-Martinez M, et al. Clinical Characteristics and Outcomes of Intravenous Inotropic Therapy in Advanced Heart Failure. Circ Heart Fail 2015;8:880–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
