

Rate of Correction of Hypernatremia and Health Outcomes in Critically Ill Patients
- PMID: 30948456
- PMCID: PMC6500955
- DOI: 10.2215/CJN.10640918
Rate of Correction of Hypernatremia and Health Outcomes in Critically Ill Patients
Abstract
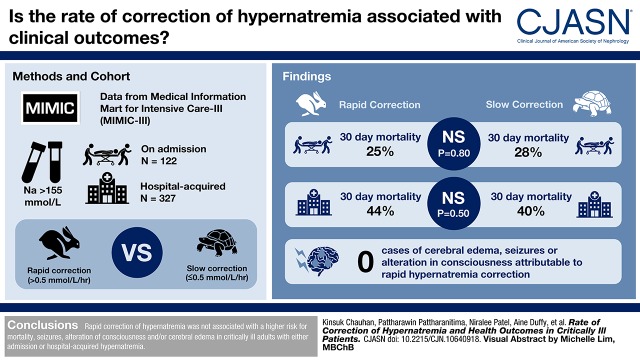
Background and objectives: Hypernatremia is common in hospitalized, critically ill patients. Although there are no clear guidelines on sodium correction rate for hypernatremia, some studies suggest a reduction rate not to exceed 0.5 mmol/L per hour. However, the data supporting this recommendation and the optimal rate of hypernatremia correction in hospitalized adults are unclear.
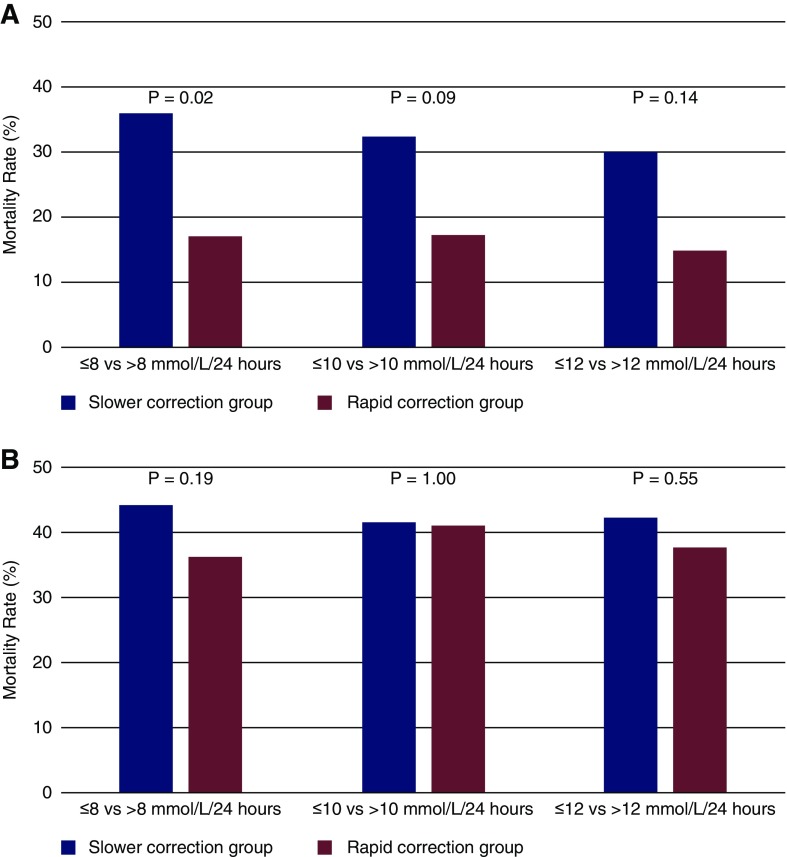
Design, setting, participants, & measurements: We assessed the association of hypernatremia correction rates with neurologic outcomes and mortality in critically ill patients with hypernatremia at admission and those that developed hypernatremia during hospitalization. We used data from the Medical Information Mart for Intensive Care-III and identified patients with hypernatremia (serum sodium level >155 mmol/L) on admission (n=122) and hospital-acquired (n=327). We calculated different ranges of rapid correction rates (>0.5 mmol/L per hour overall and >8, >10, and >12 mmol/L per 24 hours) and utilized logistic regression to generate adjusted odds ratios (aOR) with 95% confidence intervals (95% CIs) to examine association with outcomes.
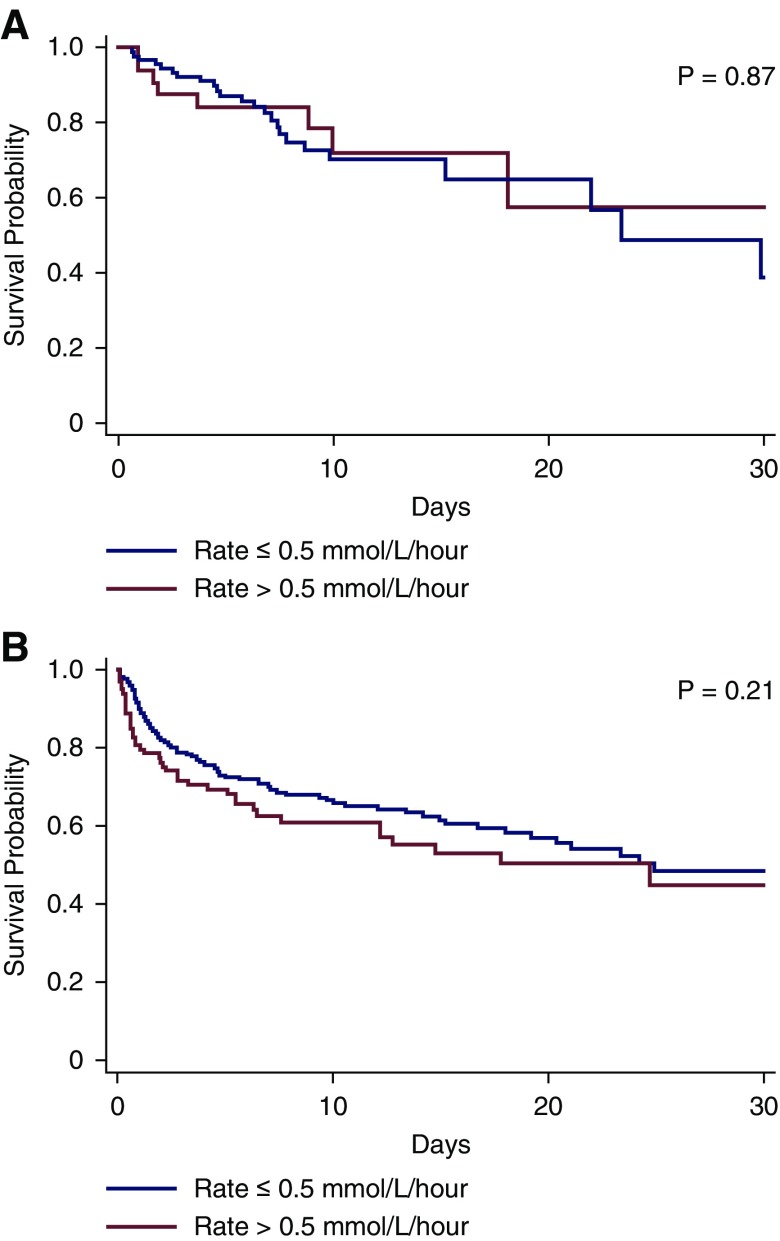
Results: We had complete data on 122 patients with severe hypernatremia on admission and 327 patients who developed hospital-acquired hypernatremia. The difference in in-hospital 30-day mortality proportion between rapid (>0.5 mmol/L per hour) and slower (≤0.5 mmol/L per hour) correction rates were not significant either in patients with hypernatremia at admission with rapid versus slow correction (25% versus 28%; P=0.80) or in patients with hospital-acquired hypernatremia with rapid versus slow correction (44% versus 40%; P=0.50). There was no difference in aOR of mortality for rapid versus slow correction in either admission (aOR, 1.3; 95% CI, 0.5 to 3.7) or hospital-acquired hypernatremia (aOR, 1.3; 95% CI, 0.8 to 2.3). Manual chart review of all suspected chronic hypernatremia patients, which included all 122 with hypernatremia at admission, 128 of the 327 hospital-acquired hypernatremia, and an additional 28 patients with ICD-9 codes for cerebral edema, seizures and/or alteration of consciousness, did not reveal a single case of cerebral edema attributable to rapid hyprnatremia correction.
Conclusions: We did not find any evidence that rapid correction of hypernatremia is associated with a higher risk for mortality, seizure, alteration of consciousness, and/or cerebral edema in critically ill adult patients with either admission or hospital-acquired hypernatremia.
Keywords: Brain Edema; Critical Care; Critical Illness; Hospital Mortality; Hospitals; Patient Admission; Sodium; hospitalization; hypernatremia; mortality; mortality risk.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
Evidence for Managing Hypernatremia: Is It Just Hyponatremia in Reverse?Clin J Am Soc Nephrol. 2019 May 7;14(5):645-647. doi: 10.2215/CJN.02950319. Epub 2019 Apr 4. Clin J Am Soc Nephrol. 2019. PMID: 31064771 Free PMC article. No abstract available.
References
-
- Adrogué HJ, Madias NE: Hypernatremia. N Engl J Med 342: 1493–1499, 2000 - PubMed
-
- Chumlea WC, Guo SS, Zeller CM, Reo NV, Siervogel RM: Total body water data for white adults 18 to 64 years of age: The Fels Longitudinal Study. Kidney Int 56: 244–252, 1999 - PubMed
-
- Palevsky PM, Bhagrath R, Greenberg A: Hypernatremia in hospitalized patients. Ann Intern Med 124: 197–203, 1996 - PubMed
-
- Funk G-C, Lindner G, Druml W, Metnitz B, Schwarz C, Bauer P, Metnitz PG: Incidence and prognosis of dysnatremias present on ICU admission. Intensive Care Med 36: 304–311, 2010 - PubMed
-
- Lindner G, Funk G-C, Schwarz C, Kneidinger N, Kaider A, Schneeweiss B, Kramer L, Druml W: Hypernatremia in the critically ill is an independent risk factor for mortality. Am J Kidney Dis 50: 952–957, 2007 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
