

Dilated Blood and Lymphatic Microvessels, Angiogenesis, Increased Macrophages, and Adipocyte Hypertrophy in Lipedema Thigh Skin and Fat Tissue
- PMID: 30949365
- PMCID: PMC6425411
- DOI: 10.1155/2019/8747461
Dilated Blood and Lymphatic Microvessels, Angiogenesis, Increased Macrophages, and Adipocyte Hypertrophy in Lipedema Thigh Skin and Fat Tissue
Abstract
Background and aim: Lipedema is a common painful SAT disorder characterized by enlargement of fat primarily in the legs of women. Case reports of lipedema tissue samples demonstrate fluid and fibrosis in the interstitial matrix, increased macrophages, and adipocyte hypertrophy. The aims of this project are to investigate blood vasculature, immune cells, and structure of lipedema tissue in a cohort of women.
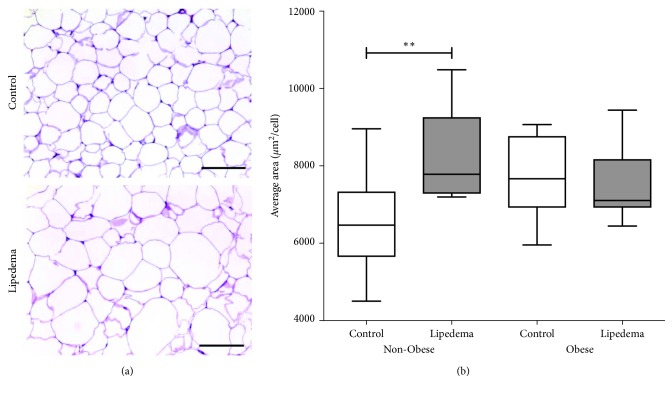
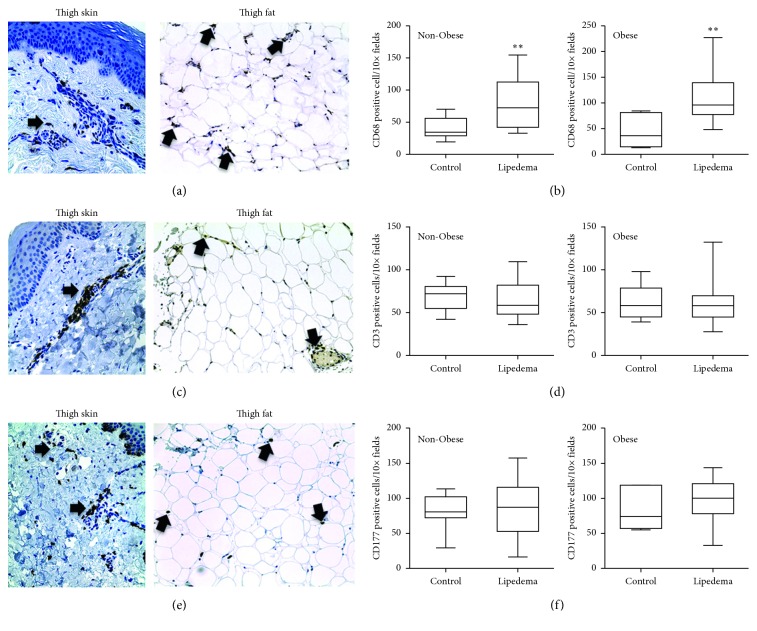
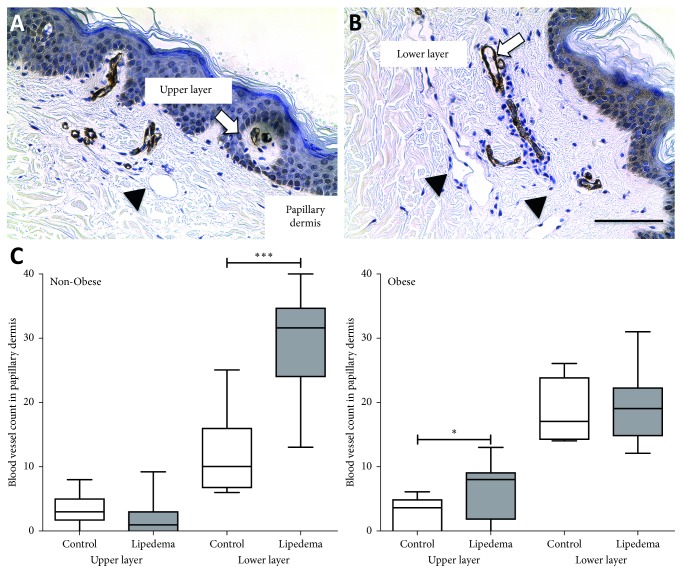
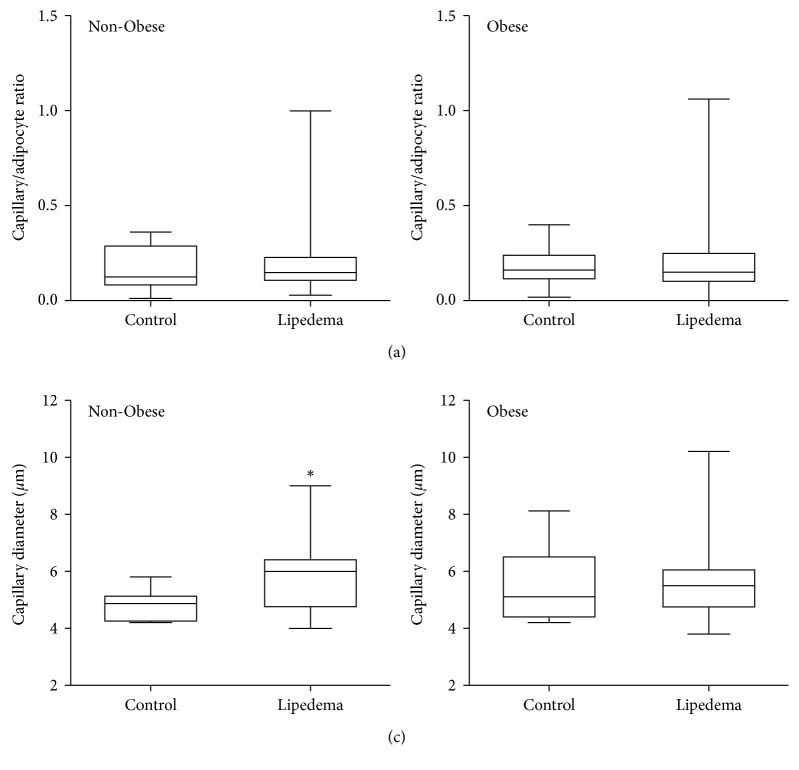
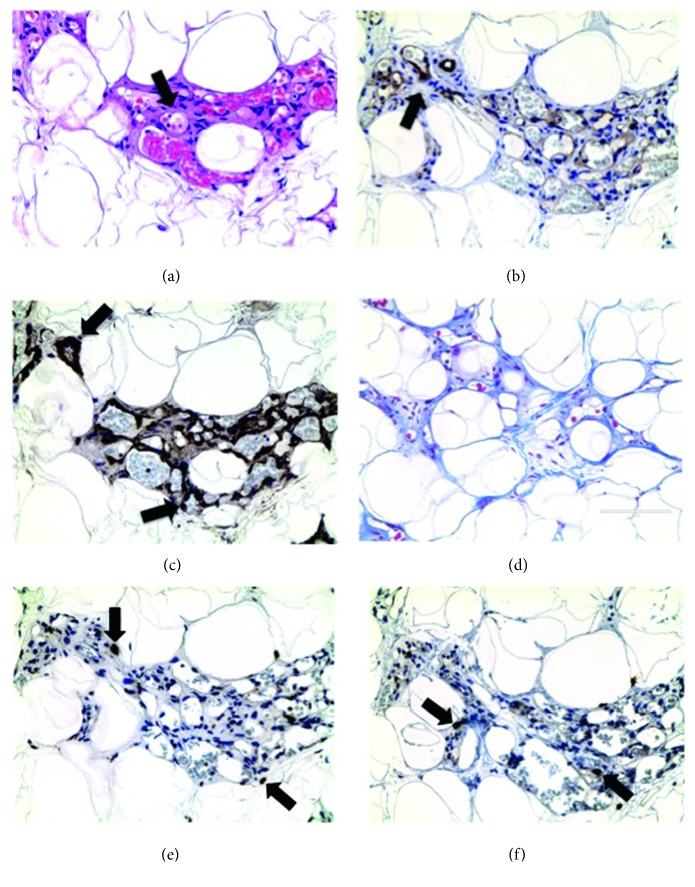
Methods: Forty-nine participants, 19 controls and 30 with lipedema, were divided into groups based on body mass index (BMI): Non-Obese (BMI 20 to <30 kg/m2) and Obese (BMI 30 to <40 kg/m2). Histological sections from thigh skin and fat were stained with H&E. Adipocyte area and blood vessel size and number were quantified using ImageJ software. Markers for macrophages (CD68), mast cells (CD117), T cells (CD3), endothelial cells (CD31), blood (SMA), and lymphatic (D2-40 and Lyve-1) vessels were investigated by IHC and IF.
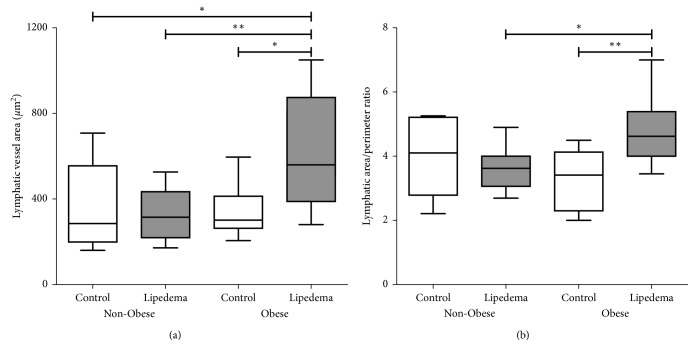
Results: Non-Obese Lipedema adipocyte area was larger than Non-Obese Controls (p=0.005) and similar to Obese Lipedema and Obese Controls. Macrophage numbers were significantly increased in Non-Obese (p < 0.005) and Obese (p < 0.05) Lipedema skin and fat compared to Control groups. No differences in T lymphocytes or mast cells were observed when comparing Lipedema to Control in both groups. SMA staining revealed increased dermal vessels in Non-Obese Lipedema patients (p < 0.001) compared to Non-Obese Controls. Lyve-1 and D2-40 staining showed a significant increase in lymphatic vessel area but not in number or perimeter in Obese Lipedema participants (p < 0.05) compared to Controls (Obese and Non-Obese). Areas of angiogenesis were found in the fat in 30% of lipedema participants but not controls.
Conclusion: Hypertrophic adipocytes, increased numbers of macrophages and blood vessels, and dilation of capillaries in thigh tissue of non-obese women with lipedema suggest inflammation, and angiogenesis occurs independent of obesity and demonstrates a role of altered vasculature in the manifestation of the disease.
Figures
References
-
- Allen E. V., Hines E. A., Jr. Lipedema of the legs: a syndrome characterised by fat legs and orthostatic edema. Proceedings of the Staff Meetings of the Mayo Clinic; 1940; Mayo Clinic, Rochester, MN, USA. pp. 184–187.
-
- Herbst K. L., Mirkovskaya L., Bharhagava A., Chava Y., Te C. H. T. Lipedema fat and signs and symptoms of illness, increase with advancing stage. Archives of Medicine. 2015;7(4–10):1–8.
-
- Cornely M. Lipoedema of arms and legs. Part 2: conservative and surgical therapy of the lipoedema, lipohyper-plasia dolorosa. Phlebologie. 2017;40:146–151.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
