

Vestibular evoked myogenic potentials in practice: Methods, pitfalls and clinical applications
- PMID: 30949613
- PMCID: PMC6430081
- DOI: 10.1016/j.cnp.2019.01.005
Vestibular evoked myogenic potentials in practice: Methods, pitfalls and clinical applications
Abstract
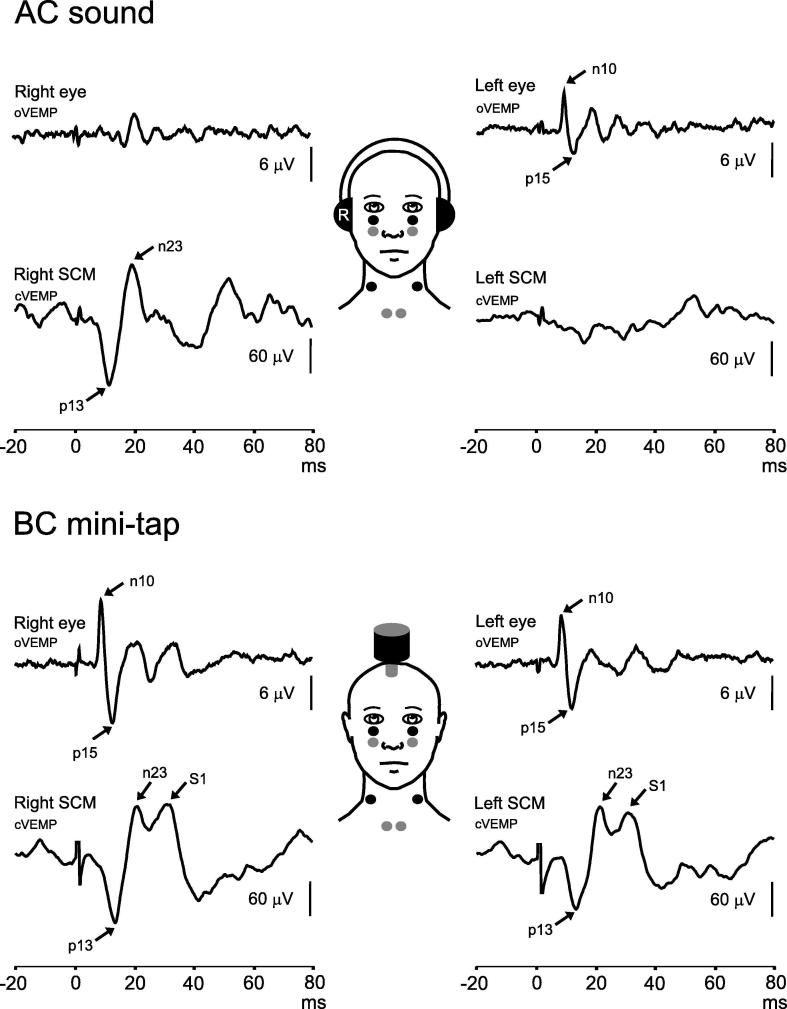
Vestibular evoked myogenic potentials (VEMPs) are a useful and increasingly popular component of the neuro-otology test battery. These otolith-dependent reflexes are produced by stimulating the ears with air-conducted sound or skull vibration and recorded from surface electrodes placed over the neck (cervical VEMPs) and eye muscles (ocular VEMPs). VEMP abnormalities have been reported in various diseases of the ear and vestibular system, and VEMPs have a clear role in the diagnosis of superior semicircular canal dehiscence. However there is significant variability in the methods used to stimulate the otoliths and record the reflexes. This review discusses VEMP methodology and provides a detailed theoretical background for the techniques that are typically used. The review also outlines the common pitfalls in VEMP recording and the clinical applications of VEMPs.
Keywords: AC, air-conducted; AR, asymmetry ratio; AVS, acute vestibular syndrome; BAER, brainstem auditory evoked potential; BC, bone-conducted; BPV, benign positioning vertigo; BVP, bilateral vestibulopathy; CANVAS, cerebellar ataxia, neuropathy and vestibular areflexia syndrome; Deg, degrees; ECG, electrocardiographic; EEG, electroencephalographic; EMG, electromyographic activity/electromyogram; FL, force level; HL, hearing level; IO, inferior oblique; MD, Meniere’s disease; Method; NIOSH, National Institutes of Occupational Safety and Health; Otolith; PCS, posterior circulation stroke; PICA, posterior inferior cerebellar artery; PP, peak-to-peak; RMS, root mean square; SCC, semicircular canal; SCD, superior canal dehiscence; SCM, sternocleidomastoid; SL, sensation level; SPL, sound pressure level, being the RMS value for a sinusoid; SVH, subjective visual horizontal; Sound; UW, unilateral weakness; VEMP; VEMP, vestibular evoked myogenic potential; VM, vestibular migraine; VN, vestibular neuritis; VS, vestibular schwannoma; Vestibular; Vibration; cVEMP, cervical vestibular evoked myogenic potential; dB, decibels, the logarithm of the relative power versus a reference; dBA, decibels, measured using an “A” weighting; nHL, normal hearing level; oVEMP, ocular vestibular evoked myogenic potential; pkFL, peak force level; pkSPL, peak sound pressure level (3 dB higher than RMS for a sinusoid); vHIT, video head impulse test.
Figures
References
-
- Aw S.T., Welgampola M.S., Bradshaw A.P., Todd M.J., Magnussen J.S., Halmagyi G.M. Click-evoked vestibulo-ocular reflex distinguishes posterior from superior canal dehiscence. Neurology. 2010;75(10):933–935. - PubMed
-
- Basta D., Todt I., Ernst A. Characterization of age-related changes in vestibular evoked myogenic potentials. J. Vestib. Res. 2007;17(2–3):93–98. - PubMed
-
- Brantberg K. Familial early-onset progressive vestibulopathy without hearing impairment. Acta Otolaryngol. 2003;123(6):713–717. - PubMed
-
- Brantberg K., Tribukait A. Vestibular evoked myogenic potentials in response to laterally directed skull taps. J. Vestib. Res. 2002;12(1):35–45. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
