

Optimizing Actigraphic Estimation of Sleep Duration in Suspected Idiopathic Hypersomnia
- PMID: 30952223
- PMCID: PMC6457505
- DOI: 10.5664/jcsm.7722
Optimizing Actigraphic Estimation of Sleep Duration in Suspected Idiopathic Hypersomnia
Abstract
Study objectives: To determine the optimal Actiwatch 2 setting configuration for the estimation of total sleep time (TST) in persons with suspected idiopathic hypersomnia.
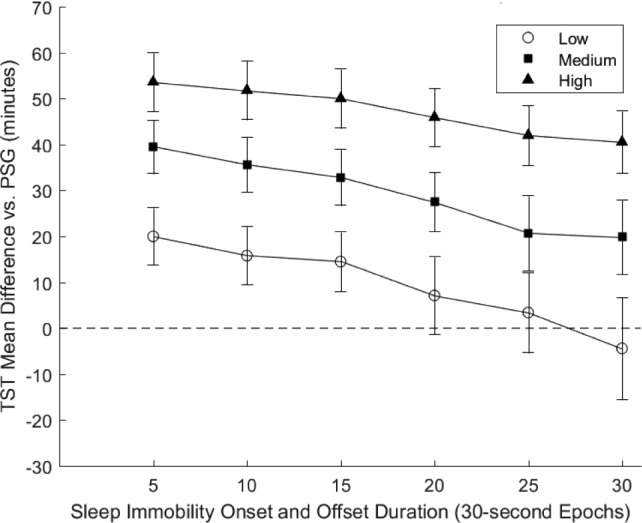
Methods: Thirty-three patients with a diagnosis of idiopathic hypersomnia (28 female; mean age = 33.7 ± 10.5) underwent ad libitum polysomnography with concurrent use of the Actiwatch 2. Actiwatch 2 sleep-wake activity threshold (SWAT; Low, Medium, and High) and sleep immobility onset and offset (SIOO; 5, 10, 15, 20, 25, and 30 epoch) duration were modified during data processing. The resultant 18 unique setting combinations were subsequently evaluated using Bland-Altman and epoch comparison analyses to determine optimal settings relative to polysomnography.
Results: Low SWAT + 25 Epoch SIOO displayed the least divergence from polysomnography (mean difference 3.4 minutes). Higher SWAT and lower SIOO increased sensitivity and accuracy, but at the expense of reducing specificity and the ability to accurately estimate TST.
Conclusions: These results demonstrate that actigraphic settings should be carefully considered when estimating sleep duration. The Low + 25 Epoch configuration is indicated as most optimal for estimating TST in persons with suspected idiopathic hypersomnia.
Commentary: A commentary on this article appears in this issue on page 539.
Keywords: Actiwatch; actigraphy; hypersomnolence; idiopathic hypersomnia.
© 2019 American Academy of Sleep Medicine.
Figures
Comment in
-
Are We There Yet? Getting Closer to Certainty in Idiopathic Hypersomnia Diagnosis.J Clin Sleep Med. 2019 Apr 15;15(4):539-540. doi: 10.5664/jcsm.7706. J Clin Sleep Med. 2019. PMID: 30952230 Free PMC article. No abstract available.
References
-
- Billiard M, Sonka K. Idiopathic hypersomnia. Sleep Med Rev. 2016;29:23–33. - PubMed
-
- Boon P, Pevernagie D, Schrans D. Hypersomnolence and narcolepsy; a pragmatic diagnostic neurophysiological approach. Acta Neurol Belg. 2002;102(1):11–18. - PubMed
-
- American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
