

Clinical and Genome-wide Analysis of Cisplatin-induced Tinnitus Implicates Novel Ototoxic Mechanisms
- PMID: 30952644
- PMCID: PMC6903403
- DOI: 10.1158/1078-0432.CCR-18-3179
Clinical and Genome-wide Analysis of Cisplatin-induced Tinnitus Implicates Novel Ototoxic Mechanisms
Abstract
Purpose: Cisplatin, a commonly used chemotherapeutic, results in tinnitus, the phantom perception of sound. Our purpose was to identify the clinical and genetic determinants of tinnitus among testicular cancer survivors (TCS) following cisplatin-based chemotherapy.
Experimental design: TCS (n = 762) were dichotomized to cases (moderate/severe tinnitus; n = 154) and controls (none; n = 608). Logistic regression was used to evaluate associations with comorbidities and SNP dosages in genome-wide association study (GWAS) following quality control and imputation (covariates: age, noise exposure, cisplatin dose, genetic principal components). Pathway over-representation tests and functional studies in mouse auditory cells were performed.
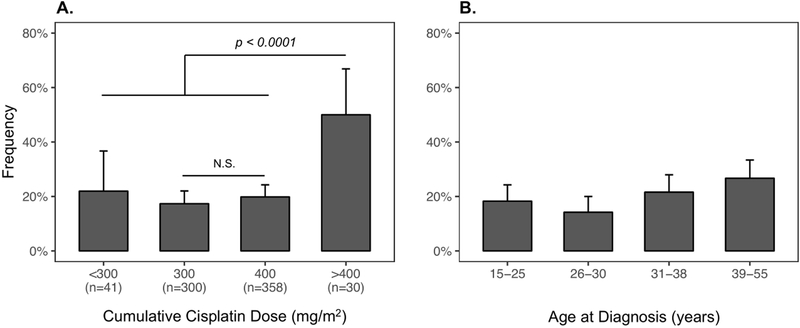
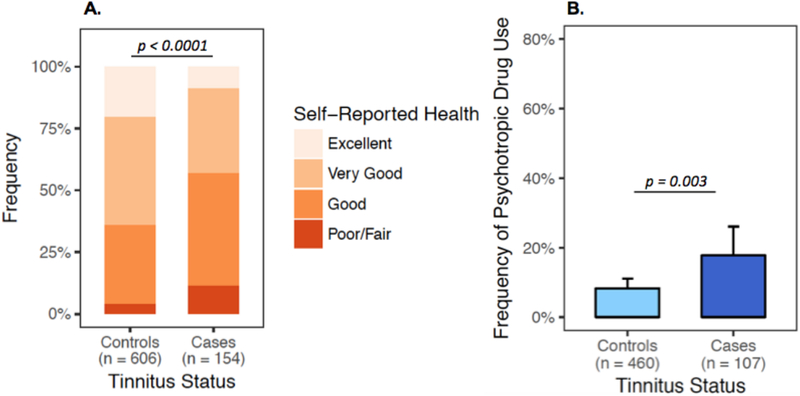
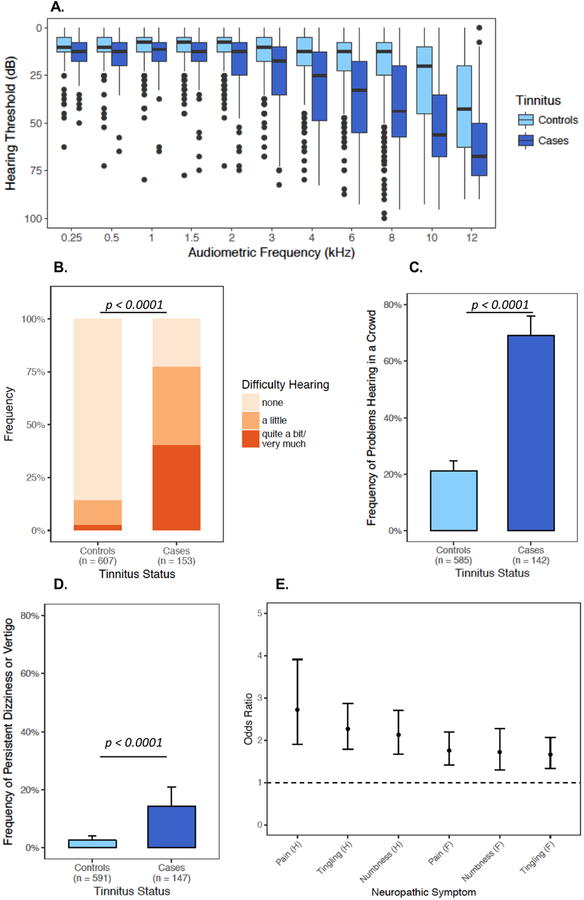
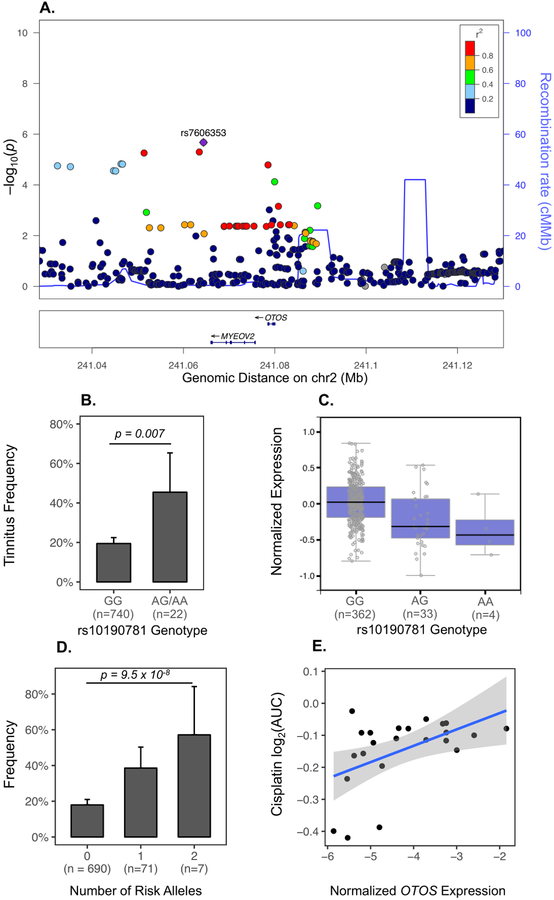
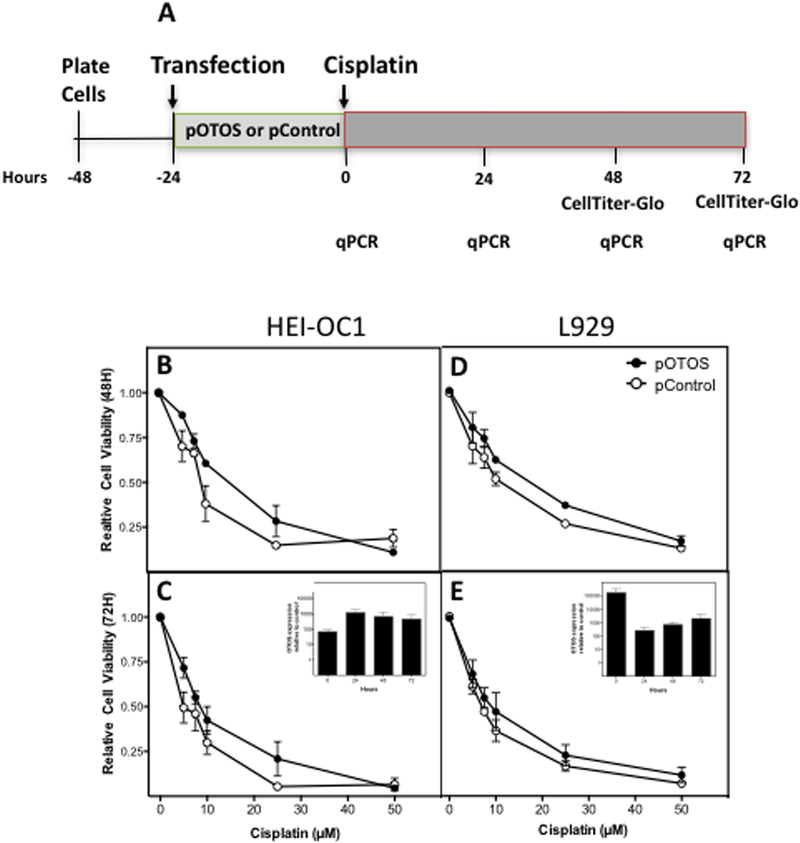
Results: Cisplatin-induced tinnitus (CisIT) significantly associated with age at diagnosis (P = 0.007) and cumulative cisplatin dose (P = 0.007). CisIT prevalence was not significantly greater in 400 mg/m2-treated TCS compared with 300 (P = 0.41), but doses >400 mg/m2 (median 580, range 402-828) increased risk by 2.61-fold (P < 0.0001). CisIT cases had worse hearing at each frequency (0.25-12 kHz, P < 0.0001), and reported more vertigo (OR = 6.47; P < 0.0001) and problems hearing in a crowd (OR = 8.22; P < 0.0001) than controls. Cases reported poorer health (P < 0.0001) and greater psychotropic medication use (OR = 2.4; P = 0.003). GWAS suggested a variant near OTOS (rs7606353, P = 2 × 10-6) and OTOS eQTLs were significantly enriched independently of that SNP (P = 0.018). OTOS overexpression in HEI-OC1, a mouse auditory cell line, resulted in resistance to cisplatin-induced cytotoxicity. Pathway analysis implicated potassium ion transport (q = 0.007).
Conclusions: CisIT associated with several neuro-otological symptoms, increased use of psychotropic medication, and poorer health. OTOS, expressed in the cochlear lateral wall, was implicated as protective. Future studies should investigate otoprotective targets in supporting cochlear cells.
©2019 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest
The authors declare no potential conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
