

HER2 Positivity Predicts Unresponsiveness to EGFR-Targeted Treatment in Metastatic Colorectal Cancer
- PMID: 30952821
- PMCID: PMC6795149
- DOI: 10.1634/theoncologist.2018-0785
HER2 Positivity Predicts Unresponsiveness to EGFR-Targeted Treatment in Metastatic Colorectal Cancer
Abstract
Background: HER2 amplification is detected in 3% of patients with colorectal cancer (CRC), making tumors in the metastatic setting vulnerable to double pharmacological HER2 blockade. Preclinical findings show that it also might impair response to anti-epidermal growth factor receptor (EGFR) treatment.
Subjects and methods: Patients with KRAS exon 2 wild-type metastatic CRC underwent molecular screening of HER2 positivity by HERACLES criteria (immunohistochemistry 3+ or 2+ in ≥50% of cells, confirmed by fluorescence in situ hybridization). A sample of consecutive HER2-negative patients was selected as control. A regression modeling strategy was applied to identify predictors explaining the bulk of HER2 positivity and the association with response to previous anti-EGFR treatment.
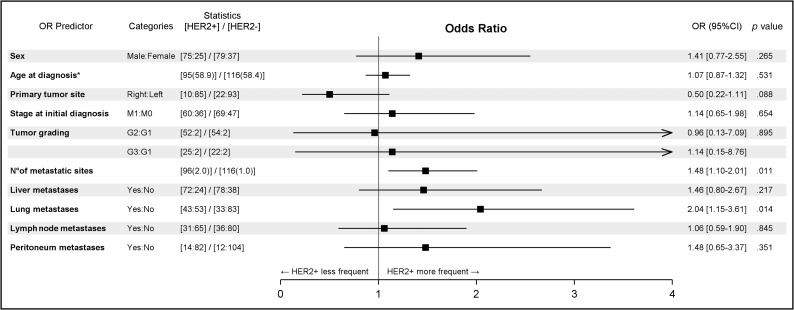
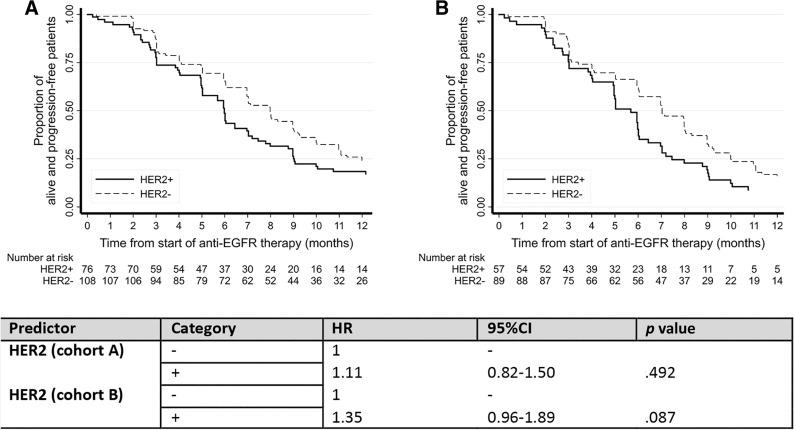
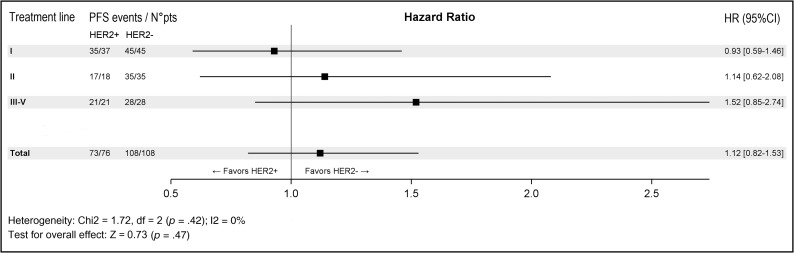
Results: From August 2012 to April 2018, a total of 100 HER2-positive metastatic CRC tumors were detected out of 1,485 KRAS exon 2 wild-type screened patients (6.7%). HER2-positive patients show more frequently lung metastases (odds ratio [OR], 2.04; 95% confidence interval [CI], 1.15-3.61; p = .014) and higher tumor burden (OR, 1.48; 95% CI, 1.10-2.01; p = .011), and tumors were more likely to be left sided (OR, 0.50; 95% CI, 0.22-1.11; p = .088). HER2-positive patients who received treatment with anti-EGFR agents (n = 79) showed poorer outcome (objective response rate, 31.2% vs. 46.9%, p = .031; progression-free survival, 5.7 months vs. 7 months, p = .087).
Conclusion: Testing for HER2 should be offered to all patients with metastatic CRC because the occurrence of this biomarker is unlikely to be predicted based on main clinicopathological features. Patients with HER2-amplified metastatic CRC are less likely to respond to anti-EGFR therapy.
Implications for practice: Patients with HER2-amplified/overexpressed metastatic colorectal cancer (mCRC) harbor a driver actionable molecular alteration that has been shown in preclinical models to hamper efficacy of the anti-epidermal growth factor receptor (EGFR) targeted therapies. The present study confirmed that this molecular feature was associated with worse objective tumor response and shorter progression-free survival in response to previous anti-EGFR therapies. Moreover, it was found that the occurrence of this biomarker is unlikely to be predicted based on main clinicopathological features. Therefore, HER2 status assessment should be included in the molecular diagnostic workup of all mCRC for speedy referral to clinical trials encompassing HER2-targeted double blockade independently of previous anti-EGFR treatment.
摘要
背景 3% 的结直肠癌 (CRC) 患者中检测到 HER2 扩增,这使得转移灶中的肿瘤容易受到双重药物 HER2 阻断。临床前研究表明,HER2 还可能损害对抗表皮生长因子受体 (EGFR) 治疗的反应。
受试者和方法 KRAS 外显子 2 野生型转移性CRC患者采用 HERACLES 标准进行 HER2 阳性分子筛查(在 ≥ 50% 的细胞中免疫组化 3 + 或 2+,经荧光原位杂交证实)。选择连续HER2 阴性患者作为对照。采用回归建模策略确定预测因素,对主要 HER2 阳性以及与先前抗 EGFR 治疗反应的相关性进行解析。
结果 2012 年 8 月至 2018 年 4 月期间,在 1 485 例 KRAS 外显子 2 野生型筛查患者中,共检测出 100 例 (6.7%) 转移性 CRC 肿瘤 HER2 阳性患者。HER2 阳性患者肺转移更频繁 [比值比 (OR), 2.04; 95% 可信区间 (CI), 1.15‐3.61; p = 0.014],肿瘤负荷较高(OR, 1.48; 95% CI, 1.10‐2.01;p = 0.011),肿瘤位于左侧的可能性更高(OR, 0.50; 95% CI,0.22‐1.11; p = 0.088)。接受抗 EGFR 药物治疗的 HER2 阳性患者 (n = 79) 预后较差(客观有效率 31.2% vs. 46.9%, p = 0.031;无进展生存期,5.7 个月 vs. 7 个月,p = 0.087)。
结论 HER2 这种生物标志物的发生不太可能根据主要的临床病理特征进行预测,故而所有转移性 CRC 患者均应接受 HER2 检测。HER 2 扩增转移性CRC 患者对抗 EGFR 治疗不太容易产生反应。
实践意义:HER2 扩增/过表达转移性结直肠癌 (mCRC) 患者存在一种驱动可操作的分子改变,临床前模型中显示出,这种改变会阻碍抗表皮生长因子受体 (EGFR) 靶向治疗的疗效。本研究证实,这一分子特征与客观肿瘤反应较差和针对之前的抗 EGFR 治疗的无进展生存时间较短有关。此外,我们还发现这种生物标志物的发生不太可能根据主要的临床病理特征进行预测。因此,所有 mCRC 的分子诊断工作都应纳入 HER2 状态评估,以便在不依赖以往抗 EGFR 治疗的情况下,快速转介到包含 HER2 靶向双重阻断的临床试验中。
Keywords: Anti‐EGFR monoclonal antibodies; Colorectal cancer; ERBB2; HER2.
© AlphaMed Press 2019.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Slamon DJ, Leyland‐Jones B, Shak S et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 2001;344:783–792. - PubMed
-
- Bang Y‐J, Van Cutsem E, Feyereislova A et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2‐positive advanced gastric or gastro‐oesophageal junction cancer (ToGA): A phase 3, open‐label, randomised controlled trial. Lancet 2010;376:687–697. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
