

Heart rate, mortality, and the relation with clinical and subclinical cardiovascular diseases: results from the Gutenberg Health Study
- PMID: 30953178
- PMCID: PMC6868108
- DOI: 10.1007/s00392-019-01466-2
Heart rate, mortality, and the relation with clinical and subclinical cardiovascular diseases: results from the Gutenberg Health Study
Abstract
Background: Higher, but also lower resting heart rate (HR), has been associated with increased cardiovascular events and mortality. Little is known about the interplay between HR, cardiovascular risk factors, concomitant diseases, vascular (endothelial) function, neurohormonal biomarkers, and all-cause mortality in the general population. Thus, we aimed to investigate these relationships in a population-based cohort.
Methods: 15,010 individuals (aged 35-74 at enrolment in 2007-2012) from the Gutenberg Health Study were analyzed. Multivariable regression modeling was used to assess the relation between the variables and conditional density plots were generated for cardiovascular risk factors, diseases, and mortality to show their dependence on HR.
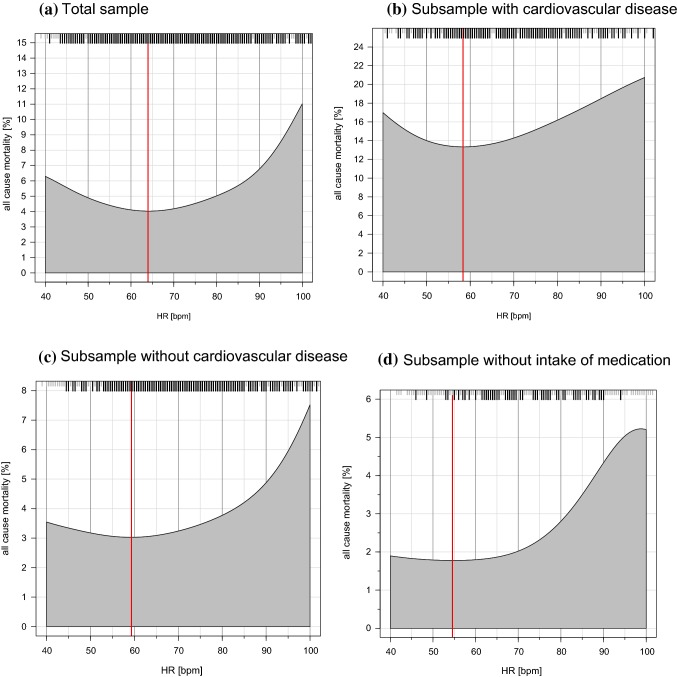
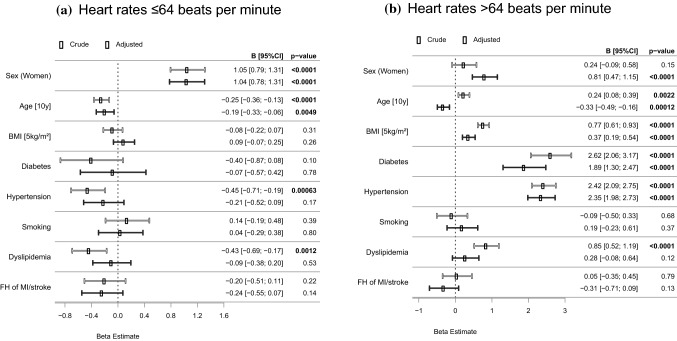
Results: There were 714 deaths in the total sample at 7.67 ± 1.68 years of follow-up. The prevalence of diabetes mellitus, arterial hypertension, coronary and peripheral artery disease, chronic heart failure, and previous myocardial infarction exhibited a J-shaped association with HR. Mortality showed a similar relation with a nadir of 64 beats per minute (bpm) in the total sample. Each 10 bpm HR reduction in HR < 64 subjects was independently associated with increased mortality (Hazard Ratio 1.36; 95% confidence interval 1.06-1.75). This increased risk was also present in HR > 64 subjects (Hazard Ratio 1.29; 95% confidence interval 1.19-1.41 per 10 bpm increase in HR). Results found for vascular and neurohormonal biomarkers exhibited a differential picture in subjects with a HR below and above the nadir.
Discussion: These results indicate that in addition to a higher HR, a lower HR is associated with increased mortality.
Keywords: Heart rate; Mortality; Neurohumoral biomarkers; Population-based; Vascular (endothelial) function.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Fox K, Ford I, Steg PG, Tendera M, Robertson M, Ferrari R, investigators B. Heart rate as a prognostic risk factor in patients with coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): a subgroup analysis of a randomised controlled trial. Lancet. 2008;372(9641):817–821. doi: 10.1016/S0140-6736(08)61171-X. - DOI - PubMed
-
- Bohm M, Swedberg K, Komajda M, Borer JS, Ford I, Dubost-Brama A, Lerebours G, Tavazzi L, Investigators S. Heart rate as a risk factor in chronic heart failure (SHIFT): the association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet. 2010;376(9744):886–894. doi: 10.1016/S0140-6736(10)61259-7. - DOI - PubMed
-
- Tardif JC, Ponikowski P, Kahan T, Investigators AS. Efficacy of the I(f) current inhibitor ivabradine in patients with chronic stable angina receiving beta-blocker therapy: a 4-month, randomized, placebo-controlled trial. Eur Heart J. 2009;30(5):540–548. doi: 10.1093/eurheartj/ehn571. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
