

Adjuvant hepatic arterial infusion pump chemotherapy and resection versus resection alone in patients with low-risk resectable colorectal liver metastases - the multicenter randomized controlled PUMP trial
- PMID: 30953467
- PMCID: PMC6451273
- DOI: 10.1186/s12885-019-5515-6
Adjuvant hepatic arterial infusion pump chemotherapy and resection versus resection alone in patients with low-risk resectable colorectal liver metastases - the multicenter randomized controlled PUMP trial
Abstract
Background: Recurrences are reported in 70% of all patients after resection of colorectal liver metastases (CRLM), in which half are confined to the liver. Adjuvant hepatic arterial infusion pump (HAIP) chemotherapy aims to reduce the risk of intrahepatic recurrence. A large retrospective propensity score analysis demonstrated that HAIP chemotherapy is particularly effective in patients with low-risk oncological features. The aim of this randomized controlled trial (RCT) --the PUMP trial-- is to investigate the efficacy of adjuvant HAIP chemotherapy in low-risk patients with resectable CRLM.
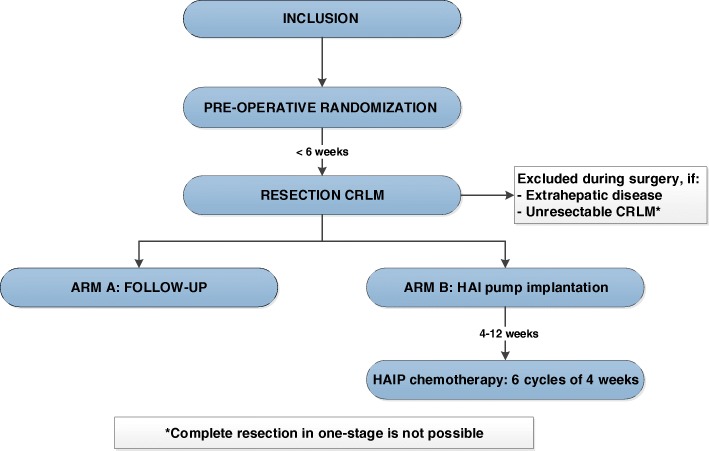
Methods: This is an open label multicenter RCT. A total of 230 patients with resectable CRLM without extrahepatic disease will be included. Only patients with a clinical risk score (CRS) of 0 to 2 are eligible, meaning: patients are allowed to have no more than two out of five poor prognostic factors (disease-free interval less than 12 months, node-positive colorectal cancer, more than 1 CRLM, largest CRLM more than 5 cm in diameter, serum Carcinoembryonic Antigen above 200 μg/L). Patients randomized to arm A undergo complete resection of CRLM without any adjuvant treatment, which is the standard of care in the Netherlands. Patients in arm B receive an implantable pump at the time of CRLM resection and start adjuvant HAIP chemotherapy 4-12 weeks after surgery, with 6 cycles of floxuridine scheduled. The primary endpoint is progression-free survival (PFS). Secondary endpoints include overall survival, hepatic PFS, safety, quality of life, and cost-effectiveness. Pharmacokinetics of intra-arterial administration of floxuridine will be investigated as well as predictive biomarkers for the efficacy of HAIP chemotherapy. In a side study, the accuracy of CT angiography will be compared to radionuclide scintigraphy to detect extrahepatic perfusion. We hypothesize that adjuvant HAIP chemotherapy leads to improved survival, improved quality of life, and a reduction of costs, compared to resection alone.
Discussion: If this PUMP trial demonstrates that adjuvant HAIP chemotherapy improves survival in low-risk patients, this treatment approach may be implemented in the standard of care of patients with resected CRLM since adjuvant systemic chemotherapy alone has not improved survival.
Trial registration: The PUMP trial is registered in the Netherlands Trial Register (NTR), number: 7493 . Date of registration September 23, 2018.
Keywords: Adjuvant chemotherapy; Colorectal liver metastasis; Hepatic arterial infusion; Resection; Survival.
Conflict of interest statement
Ethics approval and consent to participate
The protocol has been approved by the Institutional Review Board (METC Erasmus MC Rotterdam, The Netherlands). The ethical approval numbers include 362,316 (Erasmus MC, Antoni van Leeuwenhoek, Amsterdam UMC (AMC), UMC Utrecht) and 367,709 (IJsselland Hospital).
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
-
- Nordlinger B, Sorbye H, Glimelius B, Poston GJ, Schlag PM, Rougier P, et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC intergroup trial 40983): a randomised controlled trial. Lancet. 2008;371(9617):1007–1016. doi: 10.1016/S0140-6736(08)60455-9. - DOI - PMC - PubMed
-
- Nordlinger B, Sorbye H, Glimelius B, Poston GJ, Schlag PM, Rougier P, et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013;14(12):1208–1215. doi: 10.1016/S1470-2045(13)70447-9. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
