

Can the effects of the mobilization of vulnerable elders in Ontario (MOVE ON) implementation be replicated in new settings: an interrupted time series design
- PMID: 30953475
- PMCID: PMC6451288
- DOI: 10.1186/s12877-019-1124-0
Can the effects of the mobilization of vulnerable elders in Ontario (MOVE ON) implementation be replicated in new settings: an interrupted time series design
Abstract
Background: Bed rest for older hospitalized patients places them at risk for hospital-acquired morbidity. We previously evaluated an early mobilization intervention and found it to be effective at improving mobilization rates and decreasing length of stay on internal medicine units. The aim of this study was to conduct a replication study evaluating the impact of the evidence-informed mobilization intervention on surgery, psychiatry, medicine, and cardiology inpatient units.
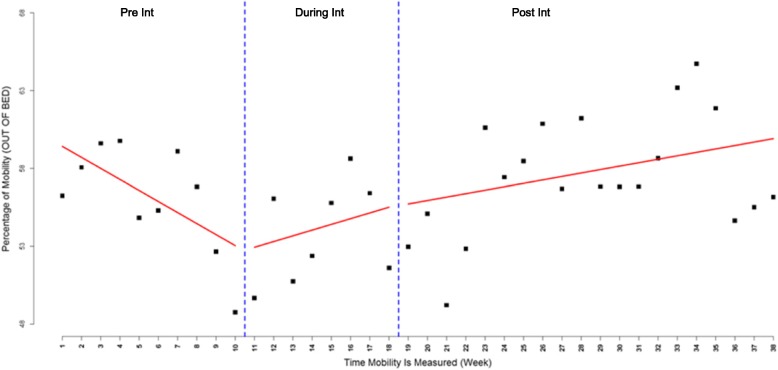
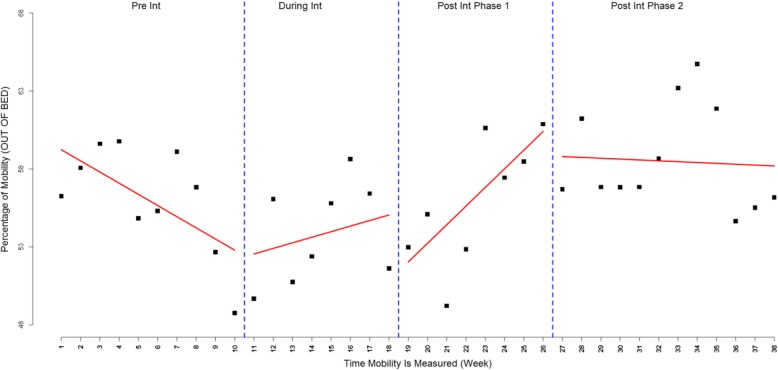
Methods: A multi-component early mobilization intervention was tailored to the local context at seven hospitals in Ontario, Canada. The primary outcome was patient mobilization measured by conducting visual audits twice a week, three times a day. Secondary outcomes were hospital length of stay and discharge destination, which were obtained from hospital decision support data. The study population was patients aged 65 years and older who were admitted to surgery, psychiatry, medicine, and cardiology inpatient units between March and August 2014. Using an interrupted time series design, the intervention was evaluated over three time periods-pre-intervention, during, and post-intervention.
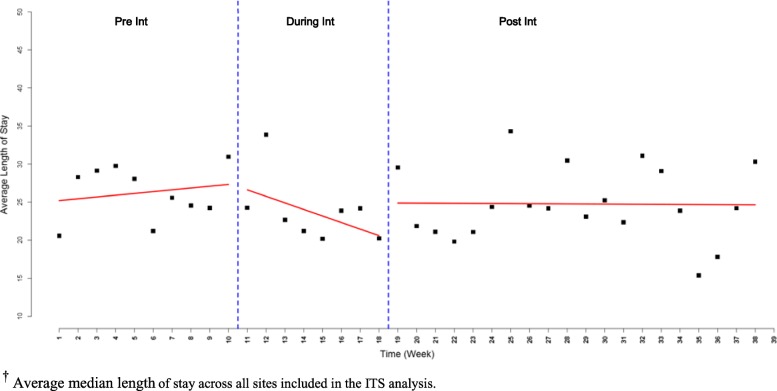
Results: A total of 3098 patients [mean age 78.46 years (SD 8.38)] were included in the overall analysis. There was a significant increase in mobility immediately after the intervention period compared to pre-intervention with a slope change of 1.91 (95% confidence interval [CI] 0.74-3.08, P-value = 0.0014). A decreasing trend in median length of stay was observed in the majority of the participating sites. Overall, a median length of stay of 26.24 days (95% CI 23.67-28.80) was observed pre-intervention compared to 23.81 days (95% CI 20.13-27.49) during the intervention and 24.69 days (95% CI 22.43-26.95) post-intervention. The overall decrease in median length of stay was associated with the increase in mobility across the sites.
Conclusions: MOVE increased mobilization and these results were replicated across surgery, psychiatry, medicine, and cardiology inpatient units.
Keywords: MOVE; Mobility; Mobilization; Older adults.
Conflict of interest statement
Ethics approval and consent to participate
The protocol was approved by the Research Ethics Board at each participating Hospital. Research Ethics Board (REB) of St. Michael’s Hospital (REB# 11–261), Toronto, Ontario, Canada. The need for informed consent of all enrolled participants was waived due to the retrospective nature of this study. However, consent was required and obtained from particpants who participated in focus groups and interviews.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Trends in aging--United States and worldwide. MMWR Morb Mortal Wkly Rep. 2003;52(6):101–104, 106. - PubMed
-
- Covinsky KE, Palmer RM, Fortinsky RH, Counsell SR, Stewart AL, Kresevic D, Burant CJ, Landefeld CS. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: increased vulnerability with age. J Am Geriatr Soc. 2003;51(4):451–458. doi: 10.1046/j.1532-5415.2003.51152.x. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
