

Review of Acute Treatment of Migraine Trial Results With the New FDA Endpoints: Design Implications for Future Trials
- PMID: 30953576
- PMCID: PMC6593965
- DOI: 10.1111/head.13511
Review of Acute Treatment of Migraine Trial Results With the New FDA Endpoints: Design Implications for Future Trials
Erratum in
-
Erratum.Headache. 2019 Sep;59(8):1427. doi: 10.1111/head.13592. Epub 2019 Jul 12. Headache. 2019. PMID: 31529475 Free PMC article. No abstract available.
Abstract
Background: In October 2014, the US Food and Drug Administration released a draft guidance for the development of drugs for the acute treatment of migraine. This guidance offered the option of replacing the previously required 4 co-primary endpoints: pain freedom, freedom from nausea, freedom from photophobia, and freedom from phonophobia, all at 2 hours posttreatment, with 2 co-primary endpoints: pain freedom and freedom from most bothersome symptom (MBS) other than pain, both at 2 hours posttreatment. At the time the new draft guidance was released, no large clinical trials had been undertaken with these 2 co-primary endpoints, posing a challenge in determining the sample size that might be required to achieve statistical significance. As a number of trials have now been completed, we conducted a review of the observed placebo responses, drug effect sizes, and sample sizes to better inform the design of future trials.
Methods: We searched PubMed, Embase, Web of Science, and the Cochrane library for primary publications of phase 3 randomized, placebo-controlled, double-blind acute migraine treatment trials that used pain freedom and MBS freedom as primary or planned secondary endpoints. For each endpoint, placebo response rates were determined and used to generate estimates of sample size, assuming differences between placebo and active treatment groups of 10%, 15%, and 20%. Sample size calculations were based on 80% power using a 2-group continuity corrected chi-square test with a 5% 2-sided significance level.
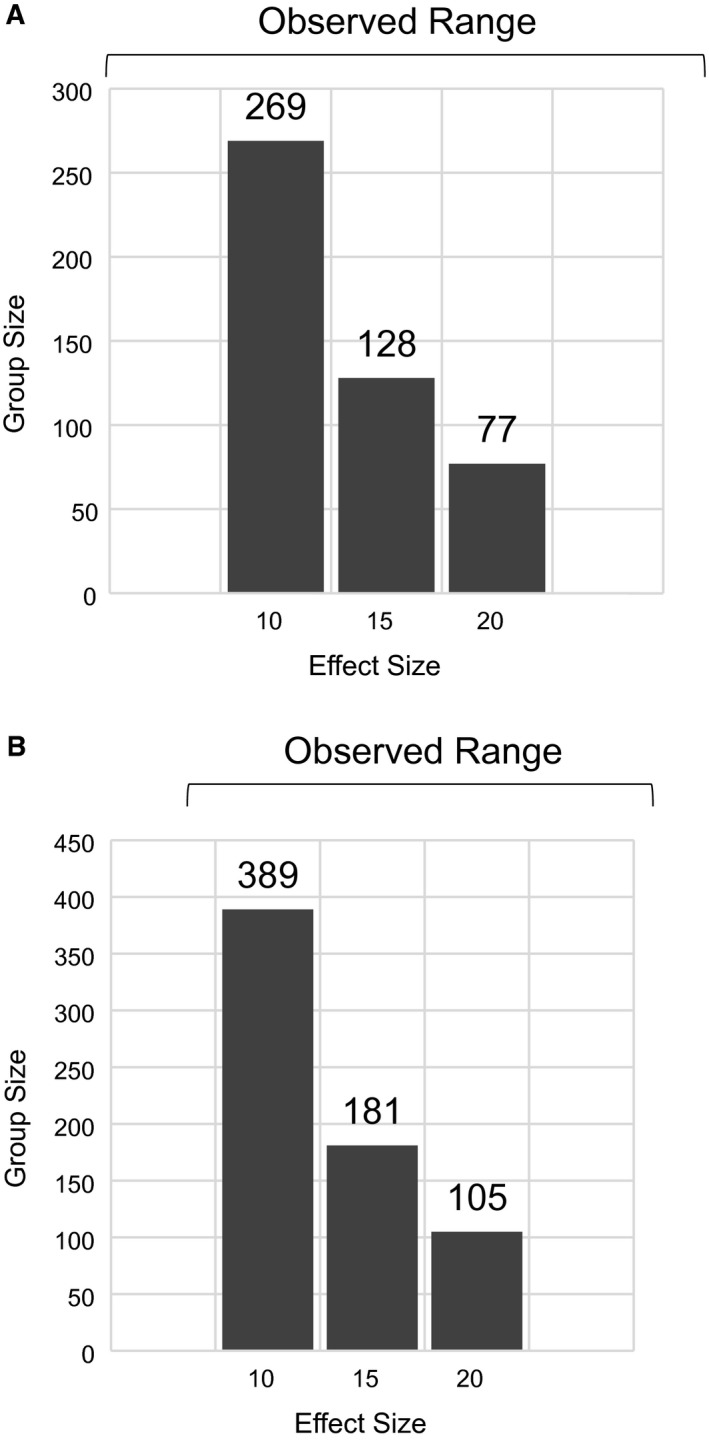
Results: We identified abstracts or full-length papers describing results of 8 clinical trials employing the new co-primary endpoints. The mean placebo response rate for 2-hour pain freedom was 16.75% (range 11.8-21.3%) and treatment effect (difference in response rates between active and placebo groups) ranged from 5.0% to 27.2%. For 2-hour MBS freedom, the mean placebo response rate was 32.8% (range 25.2-48.1%), and the range of treatment effect was 8.9% to 25.4%. Based on a placebo response rate of 17% for pain freedom, the sample sizes that would have been required to achieve statistical significance were n = 269, n = 128, and n = 77, for treatment effect sizes of 10%, 15%, and 20%, respectively. For MBS, assuming a placebo response rate of 33%, the corresponding required sample sizes would have been n = 389, n = 181, and n = 105.
Conclusions: The observed range of placebo response and treatment effect sizes suggests that use of the newly recommended 2 co-primary endpoints could reduce the sample sizes required to achieve significance compared with past trials using 4 primary endpoints (in which mean and median group sizes for recent trials were 375 and 362, respectively). However, the initial trials using the newly recommended co-primary endpoints tended to treat more participants than would have been minimally required. We anticipate that with the growing body of information regarding the use of these new endpoints, samples sizes may be more aligned with treatment efficacy, enabling faster and more cost-effective trials for acute migraine treatment.
Keywords: headache; migraine; most bothersome symptom; trial endpoints.
© 2019 The Authors. Headache: The Journal of Head and Face Pain published by Wiley Periodicals, Inc. on behalf of American Headache Society.
Figures
References
-
- Migraine: Developing Drugs for Acute Treatment Guidance for Industry. Available at https://www.fda.gov/downloads/drugs/guidances/ucm419465.pdf.
-
- Lipton RB, Grosberg B, Singer RP, et al. Efficacy and tolerability of a new powdered formulation of diclofenac potassium for oral solution for the acute treatment of migraine: Results from the International Migraine Pain Assessment Clinical Trial (IMPACT). Cephalalgia. 2010;30:1336‐1345. - PubMed
-
- Aurora SK, Silberstein SD, Kori SH, et al. MAP0004, orally inhaled DHE: A randomized, controlled study in the acute treatment of migraine. Headache. 2011;51:507‐517. - PubMed
-
- Brandes JL, Kudrow D, Stark SR, et al. Sumatriptan‐naproxen for acute treatment of migraine: A randomized trial. JAMA. 2007;297:1443‐1454. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
