

Systematic review and meta-analysis of propofol versus barbiturates for controlling refractory status epilepticus
- PMID: 30954065
- PMCID: PMC6451279
- DOI: 10.1186/s12883-019-1281-y
Systematic review and meta-analysis of propofol versus barbiturates for controlling refractory status epilepticus
Abstract
Background: Several studies have compared the efficacy and safety of propofol and barbiturates in the treatment of refractory status epilepticus (RSE). This study aims to quantitatively assess the advantages and disadvantages of propofol and barbiturates in controlling RSE.
Methods: We searched for studies with relevant data from the PubMed, Embase, Ovid, Cochrane Library, Springer Link, Web of Science, and China National Knowledge Infrastructure databases. By calculating odds ratios and standardized mean differences with 95% confidence intervals, we assessed the disease control rate (DCR), case fatality rate (CFR), average control time (ACT), average tracheal intubation placement time (ATIPT), and incidence of hypotension between propofol and barbiturates in treating RSE.
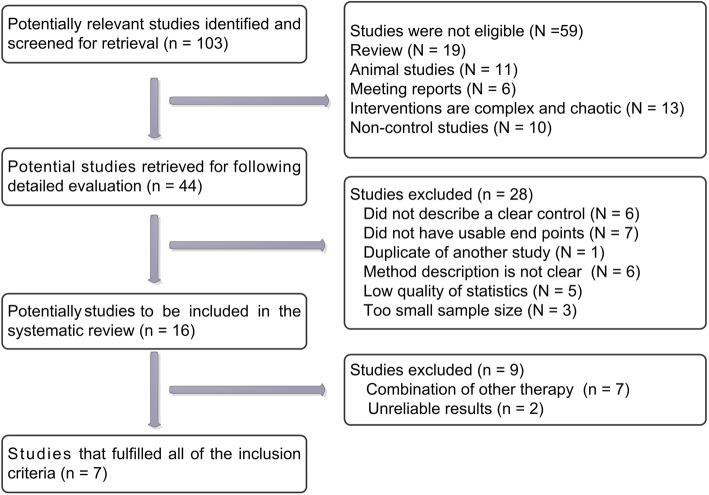
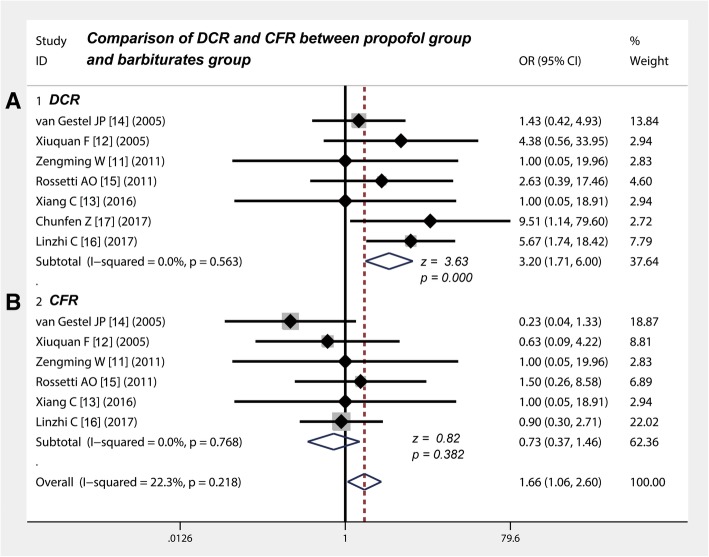
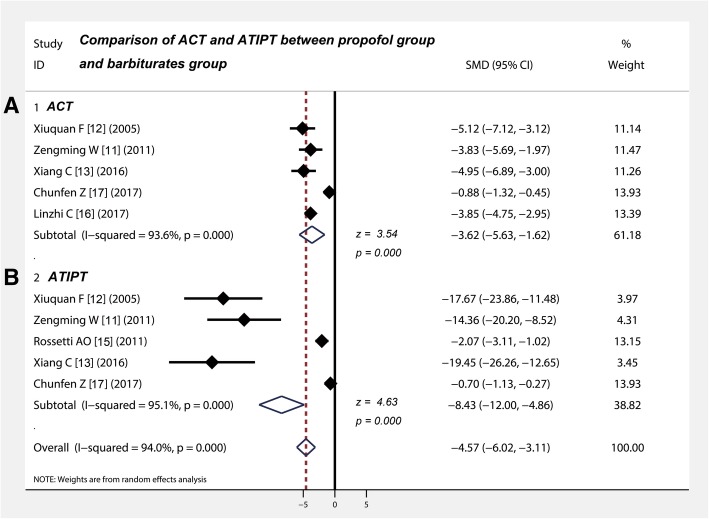
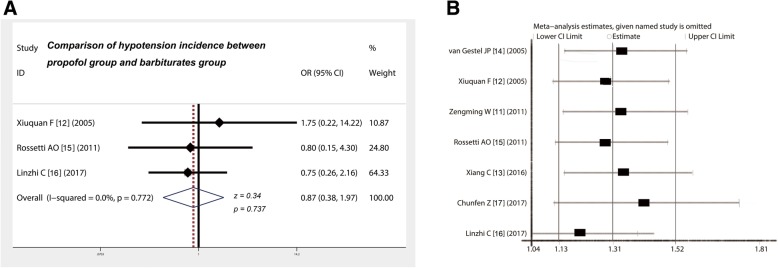
Results: Seven studies with 261 patients were included in this analysis. Meta-analysis revealed that the DCR of propofol was higher than that of barbiturates (p < 0.001) and that the CFR (p = 0.382) between the two treatment did not significantly differ in controlling RSE. Propofol shortened the ACT (p < 0.001) of RSE and reduced the ATIPT (p < 0.001) of patients with RSE more extensively than did barbiturates and did not increase the incidence of hypotension (p = 0.737).
Conclusions: In comparison with barbiturates, propofol can control RSE and shorten ATIPT in a more efficient and timely manner. Moreover, the drug does not increase the incidence of hypotension and CFR.
Keywords: Barbiturates; Meta-analysis; Propofol; RSE; Refractory status epilepticus.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval is not required for this review.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
