

Selected serum cytokines and nitric oxide as potential multi-marker biosignature panels for Parkinson disease of varying durations: a case-control study
- PMID: 30954070
- PMCID: PMC6451214
- DOI: 10.1186/s12883-019-1286-6
Selected serum cytokines and nitric oxide as potential multi-marker biosignature panels for Parkinson disease of varying durations: a case-control study
Abstract
Background: Dopaminergic neuronal loss begins years before motor symptoms appear in Parkinson disease (PD). Thus, reliable biomarkers for early diagnosis and prognosis of PD are an essential pre-requisite to develop disease modifying therapies. Inflammation-derived oxidative stress is postulated to contribute to nigrostriatal degeneration. We evaluated the role of selected serum immune mediators (IFNγ, TNFα, IL-10, and NOx) in PD progression and estimated their usefulness in preclinical diagnosis.
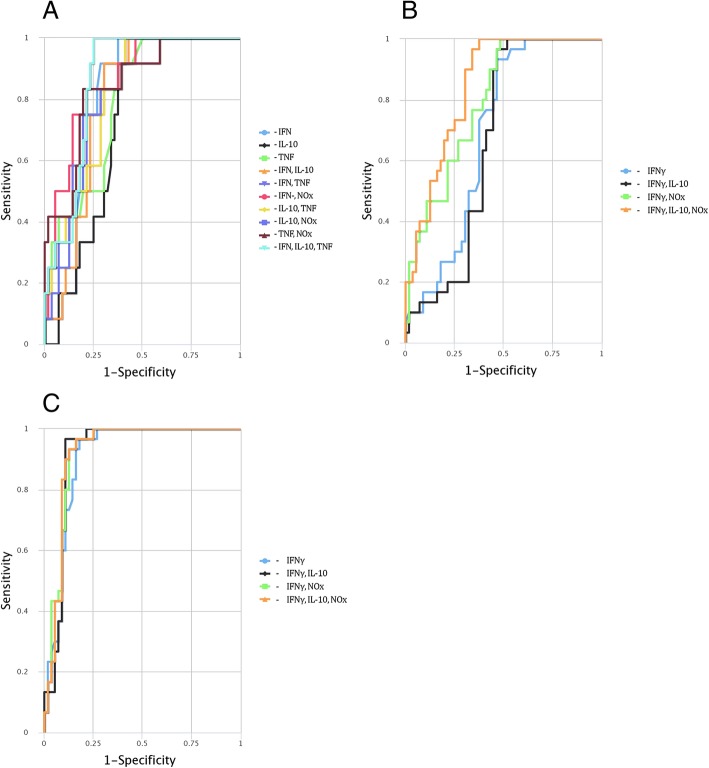
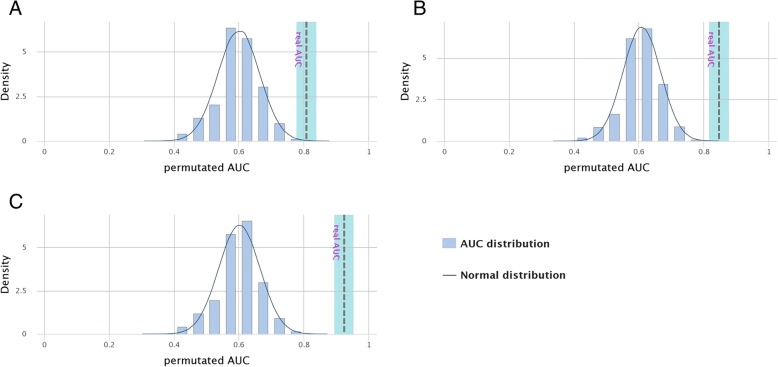
Methods: This case-control study recruited 72 PD patients with varying disease durations (< 1-year, n = 12 patients; 1-3 years, n = 30; > 3 years, n = 30) and 56 age- and gender-matched controls (26 with other neurological disorders as disease controls, and 30 healthy controls). Serum cytokine levels and NOx quantified using Sandwich Enzyme Linked Immunosorbent Assay kits, and the Griess test, respectively, were evaluated for diagnostic accuracy of optimal marker combinations by the CombiROC method. PD patients were clinically evaluated for motor and non-motor symptoms, and staged based on Hoehn and Yahr (H-Y) scale.
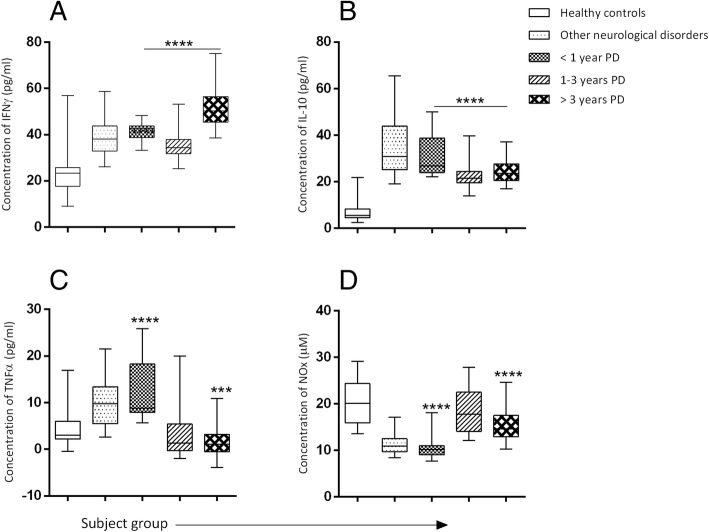
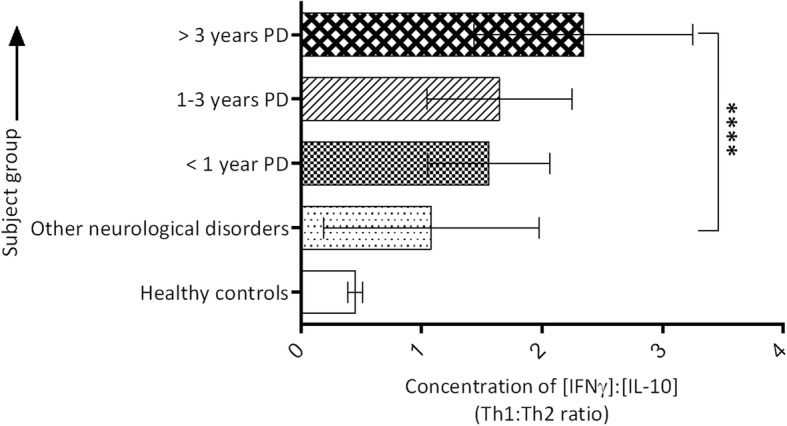
Results: A significant increase in serum IFNγ and IL-10 was observed in PD compared to healthy controls (p < 0.001). The Th1: Th2 (IFNγ: IL-10) cytokine ratio was higher in PD of 3-12 years compared with PD < 1 year (p < 0.001). Highest levels of NOx manifested during early PD (1-3 years) through a subsequent decline with disease duration. TNFα level was highest at PD onset. A low serum NOx level was associated with cognitive impairment (p = 0.002). The potential of using multi-biomarker panel, IFNγ, IL-10 and TNFα, for detection of PD onset was evident (sensitivity [SE] = 83.3%, specificity [SP] =80.4%, area under curve [AUC] = 0.868), while for early and late PD the multi-biomarker signature of IFNγ, IL-10 and NOx appeared to be more promising (SE = 93.3%, SP = 87.5%, AUC = 0.924).
Conclusion: A Th1 cytokine-biased immune response predominates with PD progression. Both IFNγ and IL-10 are involved in disease severity. However, TNFα-mediated neurotoxicity appears to occur in early PD.
Keywords: Cytokines; Nitric oxide; Parkinson disease; Serum biomarkers; Sri Lanka.
Conflict of interest statement
Ethics approval and consent to participate
The experimental procedures were approved by the Ethics Review Committee of the Faculty of Medicine, University of Colombo, Sri Lanka (ERC No. EC-16-073). Almost all subjects signed and provided voluntary informed consent before participation. In the case of a minority of patients that were unable to provide written informed consent due to their disease condition (
Consent for publication
Not applicable.
Competing interests
The author(s) declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Przedborski S. Handbook of clinical neurology. 2007. Neuroinflammation and Parkinson's disease; pp. 535–551. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
