

5-year versus risk-category-specific screening intervals for cardiovascular disease prevention: a cohort study
- PMID: 30954144
- PMCID: PMC6472327
- DOI: 10.1016/S2468-2667(19)30023-4
5-year versus risk-category-specific screening intervals for cardiovascular disease prevention: a cohort study
Abstract
Background: Clinical guidelines suggest preventive interventions such as statin therapy for individuals with a high estimated 10-year risk of major cardiovascular events. For those with a low or intermediate estimated risk, risk-factor screenings are recommended at 5-year intervals; this interval is based on expert opinion rather than on direct research evidence. Using longitudinal data on the progression of cardiovascular disease risk over time, we compared different screening intervals in terms of timely detection of high-risk individuals, cardiovascular events prevented, and health-care costs.
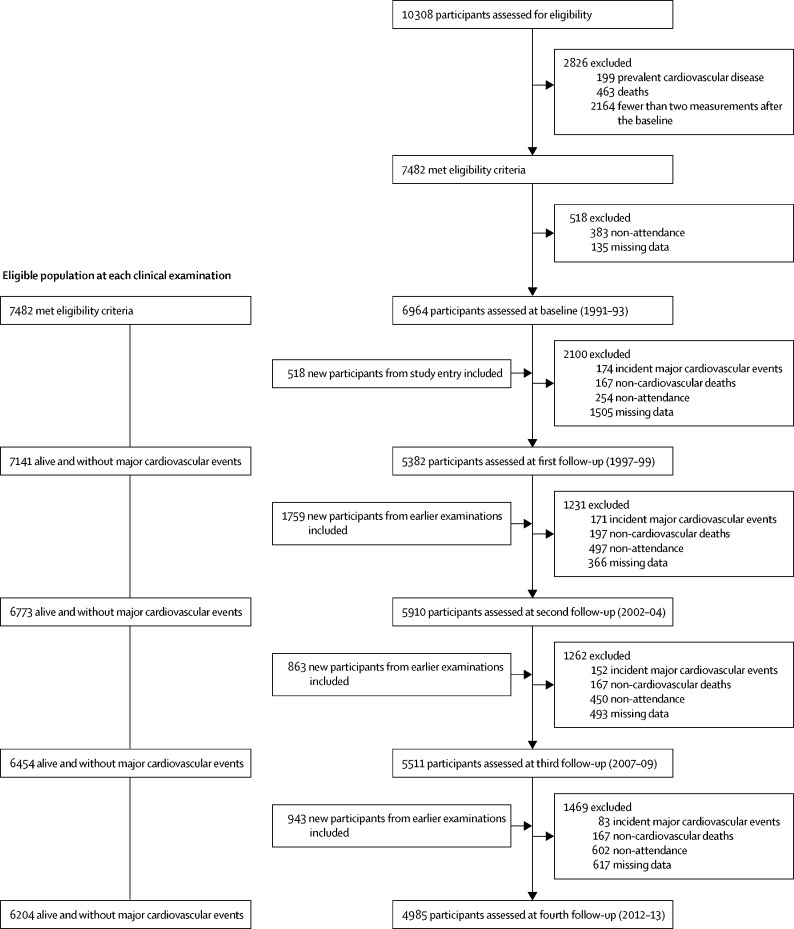
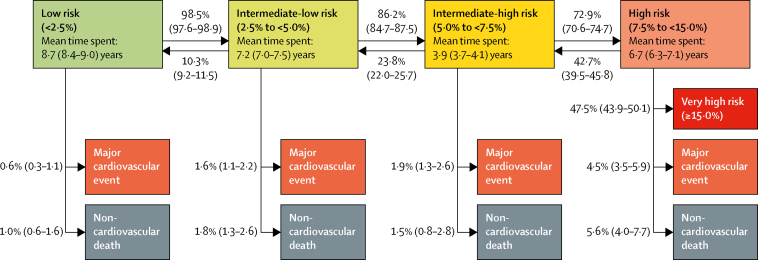
Methods: We used data from participants in the British Whitehall II study (aged 40-64 years at baseline) who had repeated biomedical screenings at 5-year intervals and linked these data to electronic health records between baseline (Aug 7, 1991, to May 10, 1993) and June 30, 2015. We estimated participants' 10-year risk of a major cardiovascular event (myocardial infarction, cardiac death, and fatal or non-fatal stroke) using the revised Atherosclerotic Cardiovascular Disease (ASCVD) calculator. We used multistate Markov modelling to estimate optimum screening intervals on the basis of progression rates from low-risk and intermediate-risk categories to the high-risk category (ie, ≥7·5% 10-year risk of a major cardiovascular event). Our assessment criteria included person-years spent in a high-risk category before detection, the number of major cardiovascular events prevented and quality-adjusted life-years (QALYs) gained, and screening costs.
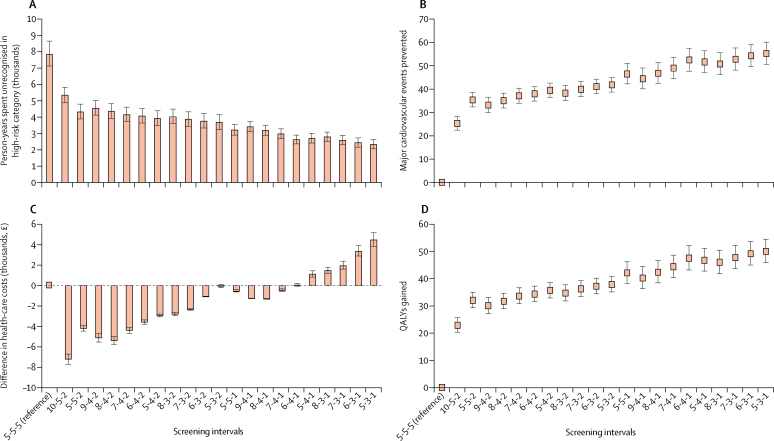
Findings: Of 6964 participants (mean age 50·0 years [SD 6·0] at baseline) with 152 700 person-years of follow-up (mean follow-up 22·0 years [SD 5·0]), 1686 participants progressed to the high-risk category and 617 had a major cardiovascular event. With the 5-year screening intervals, participants spent 7866 (95% CI 7130-8658) person-years unrecognised in the high-risk group. For individuals in the low, intermediate-low, and intermediate-high risk categories, 21 alternative risk category-based screening intervals outperformed the 5-yearly screening protocol. Screening intervals at 7 years, 4 years, and 1 year for those in the low, intermediate-low, and intermediate-high-risk category would reduce the number of person-years spent unrecognised in the high-risk group by 62% (95% CI 57-66; 4894 person-years), reduce the number of major cardiovascular events by 8% (7-9; 49 events), and raise 44 QALYs (40-49) for the study population.
Interpretation: In terms of timely preventive interventions, the 5-year screening intervals were unnecessarily frequent for low-risk individuals and insufficiently frequent for intermediate-risk individuals. Screening intervals based on risk-category-specific progression rates would perform better in terms of preventing major cardiovascular disease events and improving cost-effectiveness.
Funding: Medical Research Council, British Heart Association, National Institutes on Aging, NordForsk, Academy of Finland.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Screening interval: a public health blind spot.Lancet Public Health. 2019 Apr;4(4):e171-e172. doi: 10.1016/S2468-2667(19)30041-6. Lancet Public Health. 2019. PMID: 30954137 No abstract available.
References
-
- Ministry of Health . Ministry of Health; Wellington, New Zealand: 2018. Cardiovascular disease risk assessment and management for primary care.
-
- Piepoli MF, Hoes AW, Agewall S. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts). Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR) Eur Heart J. 2016;37:2315–2381. - PMC - PubMed
-
- WHO . World Health Organization; Geneva: 2007. Prevention of cardiovascular disease: guidelines for assessment and management of cardiovascular risk.
-
- JBS3 Board Joint British Societies' consensus recommendations for the prevention of cardiovascular disease (JBS3) Heart. 2014;100(suppl 2):ii1–ii67. - PubMed
-
- Goff DC, Jr, Lloyd-Jones DM, Bennett G. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 suppl 2):S49–S73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
