

Variations in patterns of involuntary hospitalisation and in legal frameworks: an international comparative study
- PMID: 30954479
- PMCID: PMC6475657
- DOI: 10.1016/S2215-0366(19)30090-2
Variations in patterns of involuntary hospitalisation and in legal frameworks: an international comparative study
Abstract
Background: Rising annual incidence of involuntary hospitalisation have been reported in England and some other higher-income countries, but the reasons for this increase are unclear. We aimed to describe the extent of variations in involuntary annual hospitalisation rates between countries, to compare trends over time, and to explore whether variations in legislation, demographics, economics, and health-care provision might be associated with variations in involuntary hospitalisation rates.
Methods: We compared annual incidence of involuntary hospitalisation between 2008 and 2017 (where available) for 22 countries across Europe, Australia, and New Zealand. We also obtained data on national legislation, demographic and economic factors (gross domestic product [GDP] per capita, prevalence of inequality and poverty, and the percentage of populations who are foreign born, members of ethnic minorities, or living in urban settings), and service characteristics (health-care spending and provision of psychiatric beds and mental health staff). Annual incidence data were obtained from government sources or published peer-reviewed literature.
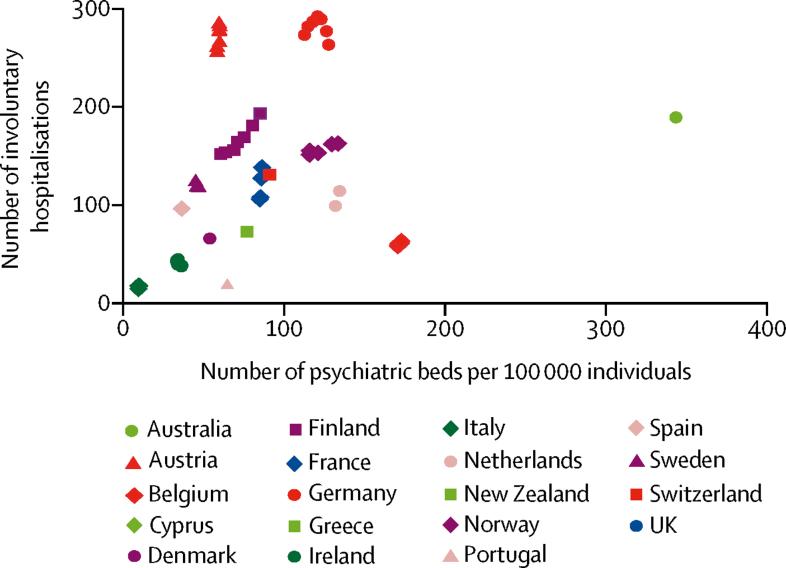
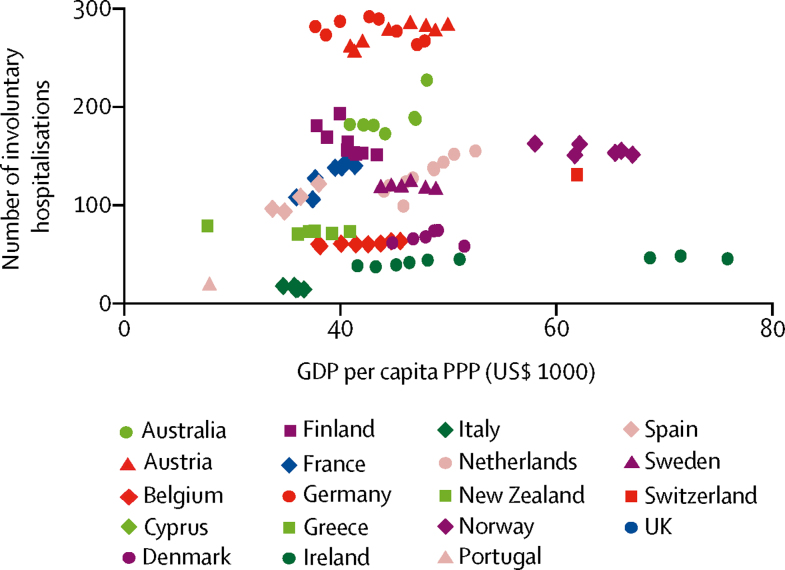
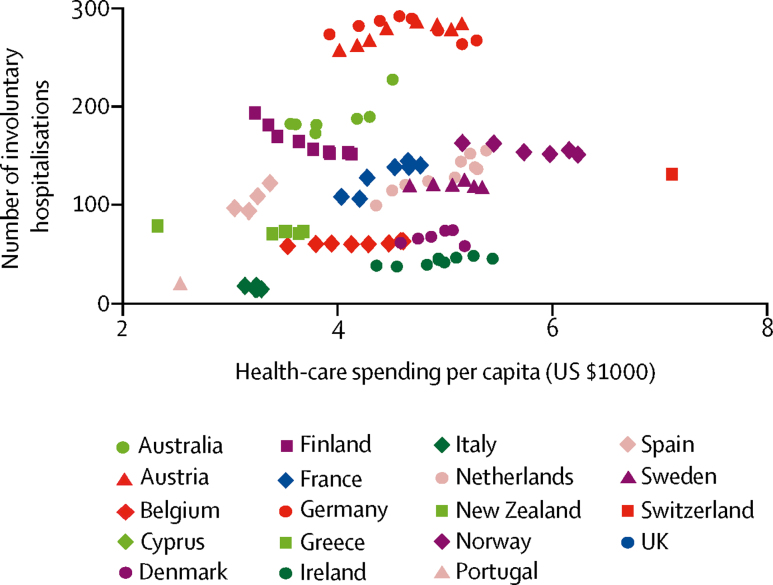
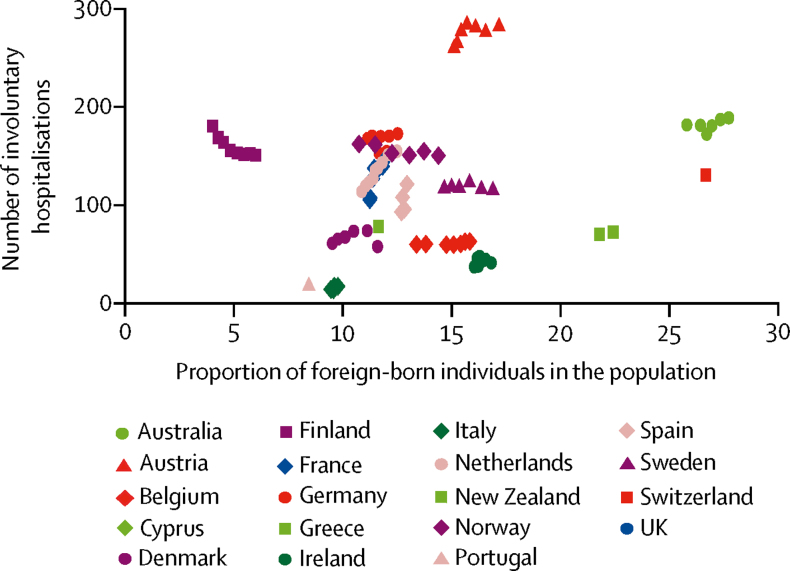
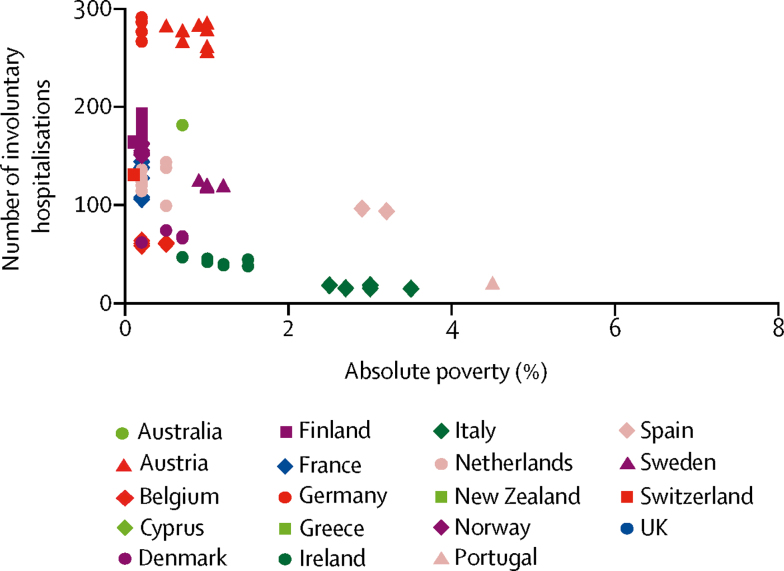
Findings: The median rate of involuntary hospitalisation was 106·4 (IQR 58·5 to 150·9) per 100 000 people, with Austria having the highest (282 per 100 000 individuals) and Italy the lowest (14·5 per 100 000 individuals) most recently available rates. We observed no relationship between annual involuntary hospitalisation rates and any characteristics of the legal framework. Higher national rates of involuntary hospitalisation were associated with a larger number of beds (β coefficient 0·65, 95% CI 0·10 to 1·20, p=0·021), higher GDP per capita purchasing power parity (β coefficient 1·84, 0·30 to 3·38, p=0·019), health-care spending per capita (β coefficient 15·92, 3·34 to 28·49, p=0·013), the proportion of foreign-born individuals in the population (β coefficient 7·32, 0·44 to 14·19, p=0·037), and lower absolute poverty (β coefficient -11·5, -22·6 to -0·3, p=0·044). There was no evidence of an association between annual involuntary hospitalisation incidence and any other demographic, economic, or health-care indicator.
Interpretation: Variations between countries were large and for the most part unexplained. We found a higher annual incidence of involuntary hospitalisation to be associated with a lower rate of absolute poverty, with higher GDP and health-care spending per capita, a higher proportion of foreign-born individuals in a population, and larger numbers of inpatient beds, but limitations in ecological research must be noted, and the associations were weak. Other country-level demographic, economic, and health-care delivery indicators and characteristics of the legislative system appeared to be unrelated to annual involuntary hospitalisation rates. Understanding why involuntary hospitalisation rates vary so much could be advanced through a more fine-grained analysis of the relationships between involuntary hospitalisation and social context, clinical practice, and how legislation is implemented in practice.
Funding: Commissioned by the Department of Health and funded by the National Institute of Health Research (NIHR) via the NIHR Mental Health Policy Research Unit.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Variations in involuntary hospitalisation across countries.Lancet Psychiatry. 2019 May;6(5):361-362. doi: 10.1016/S2215-0366(19)30095-1. Epub 2019 Apr 4. Lancet Psychiatry. 2019. PMID: 30954480 No abstract available.
-
Psychiatric bed numbers in Australia.Lancet Psychiatry. 2019 Oct;6(10):e21. doi: 10.1016/S2215-0366(19)30208-1. Lancet Psychiatry. 2019. PMID: 31544765 No abstract available.
-
Psychiatric bed numbers in Australia - Author's reply.Lancet Psychiatry. 2019 Oct;6(10):e22. doi: 10.1016/S2215-0366(19)30342-6. Lancet Psychiatry. 2019. PMID: 31544766 No abstract available.
References
-
- NHS Digital Mental Health Act Statistics, Annual Figures. 2017. https://digital.nhs.uk/data-and-information/publications/statistical/men...
-
- GOV.UK Modernising the Mental Health Act. 2018. https://assets.publishing.service.gov.uk/government/uploads/system/uploa...
-
- Salize H, Dressing H. Epidemiology of involuntary placement of mentally ill people across the European Union. Br J Psychiatr. 2004;184:163–168. - PubMed
-
- Stefano A, Ducci G. Involuntary admission and compulsory treatment in Europe: an overview. Int J Ment Health. 2008;37:10–21.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
