

Gestational age at birth and mortality from infancy into mid-adulthood: a national cohort study
- PMID: 30956154
- PMCID: PMC6691360
- DOI: 10.1016/S2352-4642(19)30108-7
Gestational age at birth and mortality from infancy into mid-adulthood: a national cohort study
Abstract
Background: Breakthroughs in the treatment of preterm birth approximately 40 years ago have enabled a generation of preterm survivors to now reach mid-adulthood. Understanding their health sequelae is essential for guiding their long-term care. We did a study to examine preterm birth in relation to mortality into mid-adulthood.
Methods: A national cohort study was done of all 4 296 814 singleton livebirths in Sweden between 1973 and 2015, who were followed up for mortality through Dec 31, 2017 (maximum age 45 years). Cox regression was used to examine gestational age at birth in relation to all-cause and cause-specific mortality, and cosibling analyses assessed for potential confounding by shared familial (genetic or environmental) factors.
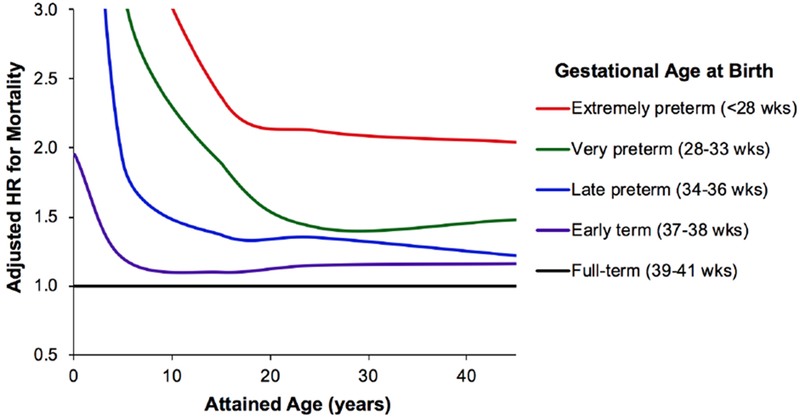
Findings: In 103·5 million person-years of follow-up, 43 916 (1·0%) deaths were reported. Gestational age at birth was inversely associated with mortality from infancy to mid-adulthood. Relative to full-term birth (39-41 weeks), the adjusted hazard ratios for mortality associated with gestational age at birth were: 66·14 (95% CI 63·09-69·34) for extremely preterm (22-27 weeks), 8·67 (8·32-9·03) for very preterm (28-33 weeks), 2·61 (2·52-2·71) for late preterm (34-36 weeks), and 1·34 (1·30-1·37) for early term (37-38 weeks), from birth to age 45 years; and 2·04 (0·92-4·55) for extremely preterm, 1·48 (1·17-1·87) for very preterm, 1·22 (1·07-1·39) for late preterm, and 1·16 (1·08-1·25) for early term, at ages 30-45 years. Preterm birth accounted for more deaths among males than females (additive interaction p<0·001). Multiple underlying causes were identified, including congenital anomalies; respiratory, endocrine, cardiovascular, and neurological diseases; cancer; and external causes. Cosibling analyses suggested that the observed associations were not due to shared genetic or environmental factors in families.
Interpretation: Preterm and early term birth should be recognised as chronic conditions that require long-term follow-up for adverse health sequelae in adulthood.
Funding: National Heart, Lung, and Blood Institute at the National Institutes of Health.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflicts of Interest:
We declare that we have no conflicts of interest.
Figures
Comment in
-
Global perspectives of premature birth across the life course.Lancet Child Adolesc Health. 2019 Jun;3(6):370-371. doi: 10.1016/S2352-4642(19)30109-9. Epub 2019 Apr 5. Lancet Child Adolesc Health. 2019. PMID: 30956153 No abstract available.
References
-
- Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet 2012; 379(9832): 2162–72. - PubMed
-
- Raju TNK, Pemberton VL, Saigal S, et al. Long-Term Healthcare Outcomes of Preterm Birth: An Executive Summary of a Conference Sponsored by the National Institutes of Health. J Pediatr 2017; 181: 309–18 e1. - PubMed
-
- Crump C, Sundquist K, Sundquist J, Winkleby MA. Gestational age at birth and mortality in young adulthood. JAMA 2011; 306(11): 1233–40. - PubMed
-
- Crump C, Sundquist K, Winkleby MA, Sundquist J. Early-term birth (37–38 weeks) and mortality in young adulthood. Epidemiology 2013; 24(2): 270–6. - PubMed
-
- Manley BJ, Doyle LW, Davies MW, Davis PG. Fifty years in neonatology. J Paediatr Child Health 2015; 51(1): 118–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
