

Meta-analysis of randomized controlled trials that assess the efficacy of low-intensity shockwave therapy for the treatment of erectile dysfunction
- PMID: 30956690
- PMCID: PMC6444401
- DOI: 10.1177/1756287219838364
Meta-analysis of randomized controlled trials that assess the efficacy of low-intensity shockwave therapy for the treatment of erectile dysfunction
Abstract
Background: The aim of this study was to perform a meta-analysis of randomized controlled trials (RCTs) that evaluate the efficacy of low-intensity extracorporeal shock wave therapy (LiESWT) for the treatment of erectile dysfunction (ED).
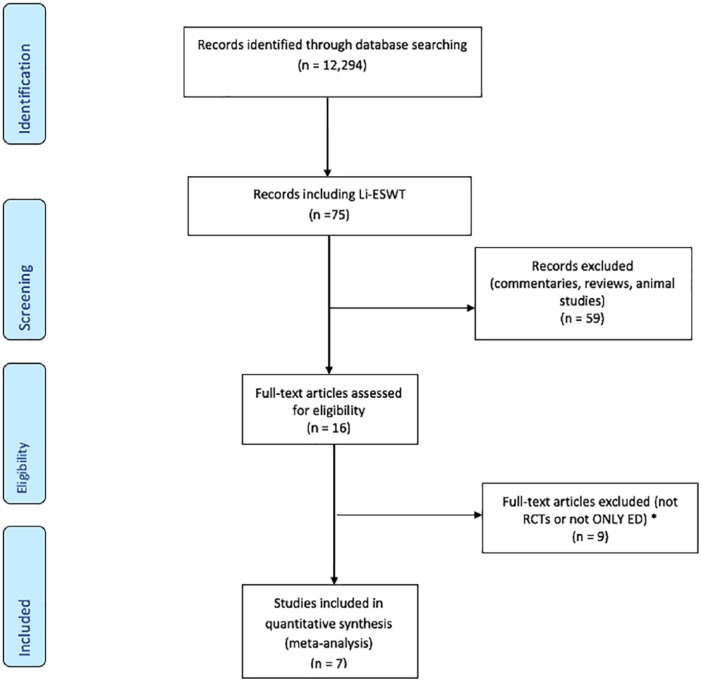
Materials and methods: A comprehensive search of PubMed, Medline, and Cochrane databases was performed from November 2005 to July 2018. RCTs evaluating efficacy of LiESWT in the treatment of ED were selected. The primary outcomes were the mean difference between treatment and sham patients in the International Index of Erectile Function-Erectile Function (IIEF-EF) domain score 1 month after treatment, and the mean change in IIEF-EF from baseline to 1 month post-treatment. The secondary analysis considered the percentage of men whose erectile hardness score (EHS) changed from <2 at baseline to >3 after treatment. All analyses used a random effects method to pool study-specific results.
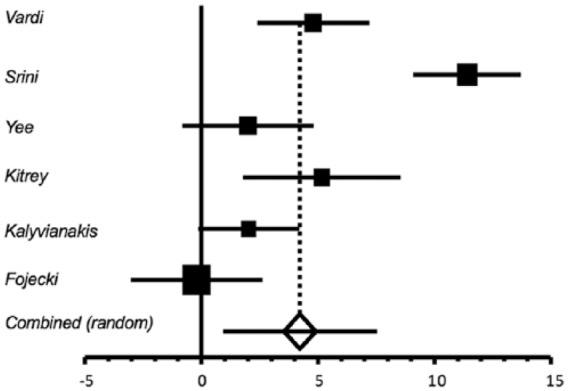
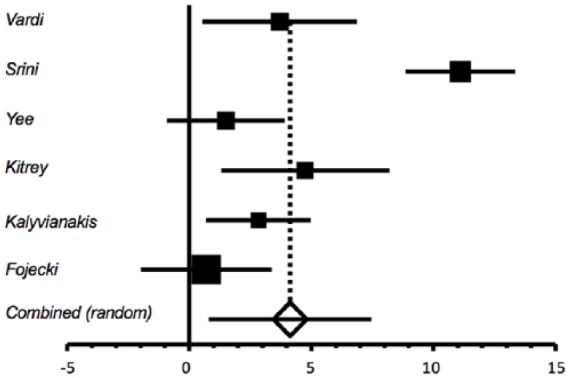
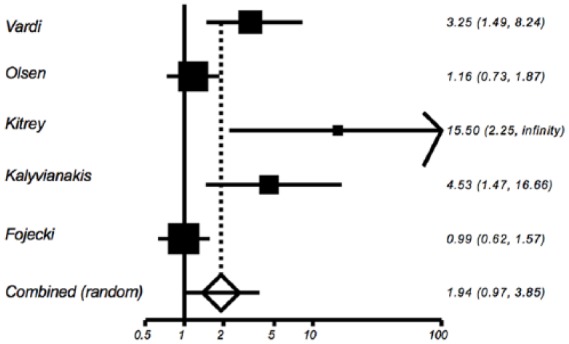
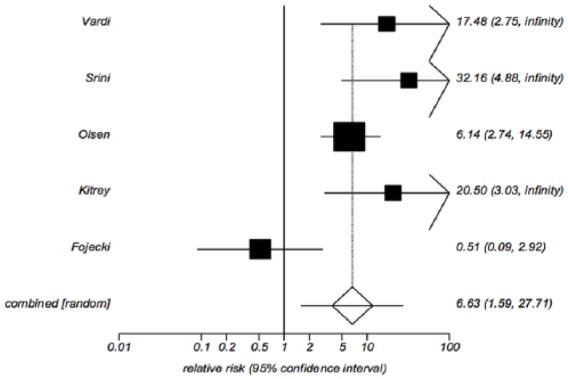
Results: A total of seven RCTs provided data for 607 patients. The mean IIEF-EF 1 month post-treatment ranged from 12.8 to 22.0 in the treatment group versus 8.17-16.43 in the sham group. The mean difference between the treatment and sham groups at the 1 month follow up was a statistically significant increase in IIEF-EF of 4.23 (p = 0.012). Overall, five of the seven trials provided data on the proportion of patients with baseline EHS <2 who improved to EHS >3 at 1 month post-treatment. The proportions ranged from 3.5 to 90% in the treatment group versus 0-9% in the sham group and the pooled relative risk of EHS improvement for the treated versus sham group was 6.63 (p = 0.0095). No significant adverse events were reported.
Conclusions: This is the first meta-analysis that evaluates RCTs exploring LiESWT as a treatment modality strictly for ED. This therapeutic strategy appears to be well tolerated with short-term benefits. However further studies exploring specific treatment regimens and long-term outcomes are needed.
Keywords: IIEF; erectile dysfunction; low-intensity extracorporeal shock wave therapy; randomized trials.
Conflict of interest statement
Conflict of interest statement: Authors I. Anusionwu and A.L. Burnett have received research grants from Medispec Ltd. The remaining authors declare no conflict of interest
Figures
References
-
- Burnett AL, Nehra A, Breau RH, et al. Erectile dysfunction: AUA guideline. J Urol 2018; 200: 633–641. - PubMed
-
- Corona G, Lee DM, Forti G, et al. Age-related changes in general and sexual health in middle-aged and older men: results from the European Male Ageing Study (EMAS). J Sex Med 2010; 7: 1362–1380. - PubMed
-
- Clavijo RI, Kohn TP, Kohn JR, et al. Effects of low-intensity extracorporeal shockwave therapy on erectile dysfunction: a systematic review and meta-analysis. J Sex Med 2017; 14: 27–35. - PubMed
-
- Lu Z, Lin G, Reed-Maldonado A, et al. Low-intensity extracorporeal shock wave treatment improves erectile function: a systematic review and meta-analysis. Eur Urol 2017; 71: 223–233. - PubMed
-
- Man L, Li G. Low-intensity extracorporeal shock wave therapy for erectile dysfunction: a systematic review and meta-analysis. Urology 2018; 119: 97–103. - PubMed
LinkOut - more resources
Full Text Sources
Medical
