

National cohort study on postoperative risks after surgery for submucosal invasive colorectal cancer
- PMID: 30957069
- PMCID: PMC6433330
- DOI: 10.1002/bjs5.50125
National cohort study on postoperative risks after surgery for submucosal invasive colorectal cancer
Abstract
Background: The decision to perform surgery for patients with T1 colorectal cancer hinges on the estimated risk of lymph node metastasis, residual tumour and risks of surgery. The aim of this observational study was to compare surgical outcomes for T1 colorectal cancer with those for more advanced colorectal cancer.
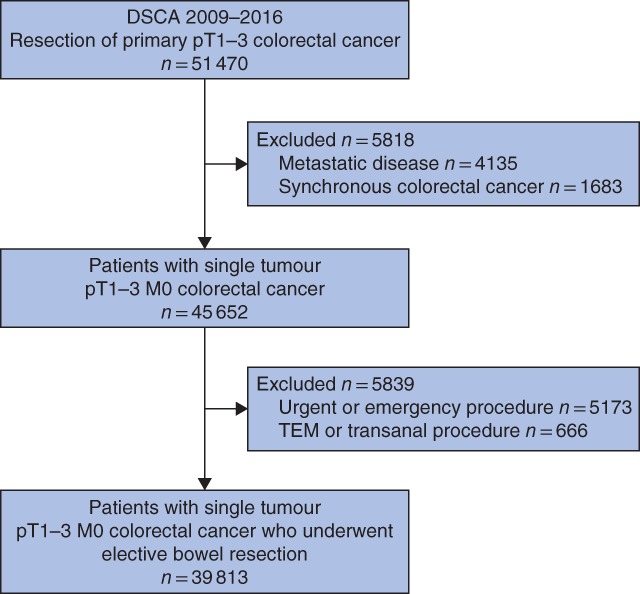
Methods: This was a population-based cohort study of patients treated surgically for pT1-3 colorectal cancer between 2009 and 2016, using data from the Dutch ColoRectal Audit. Postoperative complications (overall, surgical, severe complications and mortality) were compared using multivariable logistic regression. A risk stratification table was developed based on factors independently associated with severe complications (reintervention and/or mortality) after elective surgery.
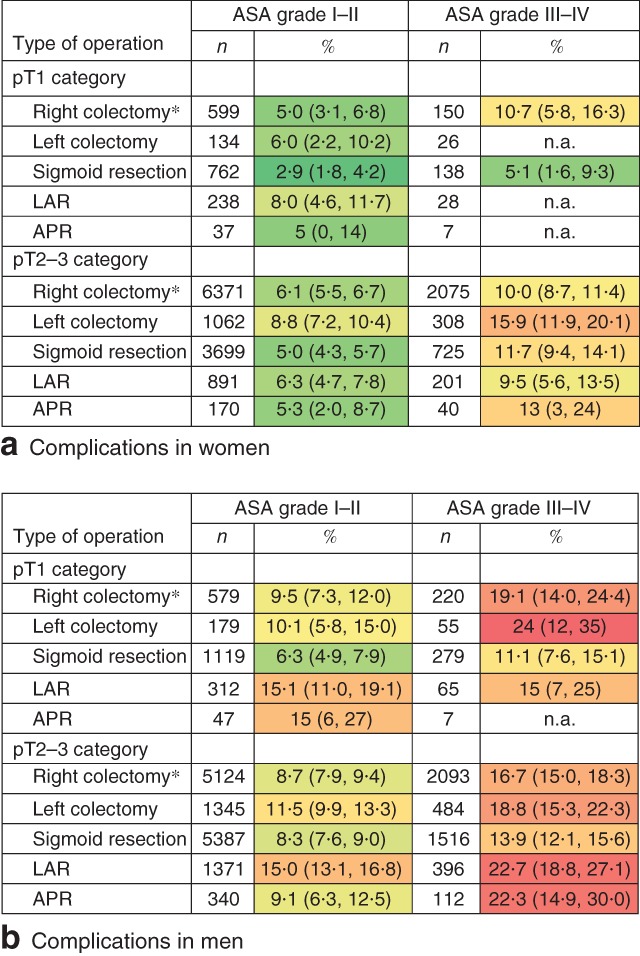
Results: Of 39 813 patients, 5170 had pT1 colorectal cancer. No statistically significant differences were observed between patients with pT1 and pT2-3 disease in the rate of severe complications (8·3 versus 9·5 per cent respectively; odds ratio (OR) 0·89, 95 per cent c.i. 0·80 to 1·01, P = 0·061), surgical complications (12·6 versus 13·5 per cent; OR 0·93, 0·84 to 1·02, P = 0·119) or mortality (1·7 versus 2·5 per cent; OR 0·94, 0·74 to 1·19, P = 0·604). Male sex, higher ASA grade, previous abdominal surgery, open approach and type of procedure were associated with a higher severe complication rate in patients with pT1 colorectal cancer.
Conclusion: Elective bowel resection was associated with similar morbidity and mortality rates in patients with pT1 and those with pT2-3 colorectal carcinoma.
Figures
References
-
- Toes‐Zoutendijk E, Kooyker AI, Elferink MA, Spaander MCW, Dekker E, Koning HJ et al; LECO working group . Stage distribution of screen‐detected colorectal cancers in the Netherlands. Gut 2018; 67: 1745–1746. - PubMed
-
- Greuter MJ, Demirel E, Lew JB, Berkhof J, Xu XM, Canfell K et al Long‐term impact of the Dutch Colorectal Cancer Screening Program on cancer incidence and mortality‐model‐based exploration of the serrated pathway. Cancer Epidemiol Biomarkers Prev 2016; 25: 135–144. - PubMed
-
- Williams JG, Pullan RD, Hill J, Horgan PG, Salmo E, Buchanan GN et al; Association of Coloproctology of Great Britain and Ireland . Management of the malignant colorectal polyp: ACPGBI position statement. Colorectal Dis 2013; 15(Suppl 2): 1–38. - PubMed
-
- Backes Y, de Vos Tot Nederveen Cappel WH, van Bergeijk J, Ter Borg F, Schwartz MP, Spanier BWM et al Risk for incomplete resection after macroscopic radical endoscopic resection of T1 colorectal cancer: a multicenter cohort study. Am J Gastroenterol 2017; 112: 785–796. - PubMed
-
- Ikematsu H, Yoda Y, Matsuda T, Yamaguchi Y, Hotta K, Kobayashi N et al Long‐term outcomes after resection for submucosal invasive colorectal cancers. Gastroenterology 2013; 144: 551–559. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
