

Bortezomib reinduction chemotherapy in high-risk ALL in first relapse: a report from the Children's Oncology Group
- PMID: 30957229
- PMCID: PMC6606340
- DOI: 10.1111/bjh.15919
Bortezomib reinduction chemotherapy in high-risk ALL in first relapse: a report from the Children's Oncology Group
Abstract
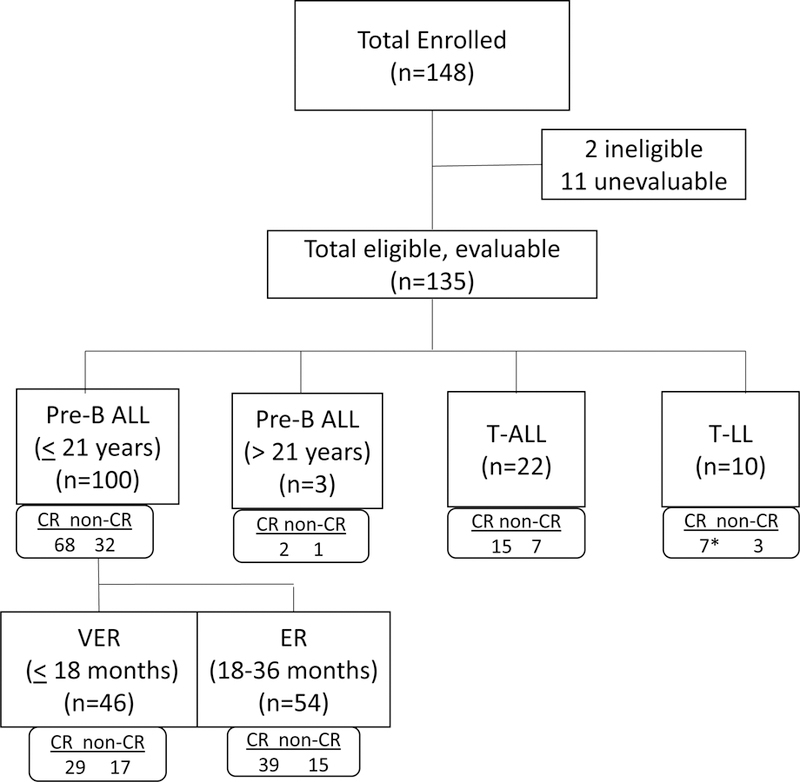
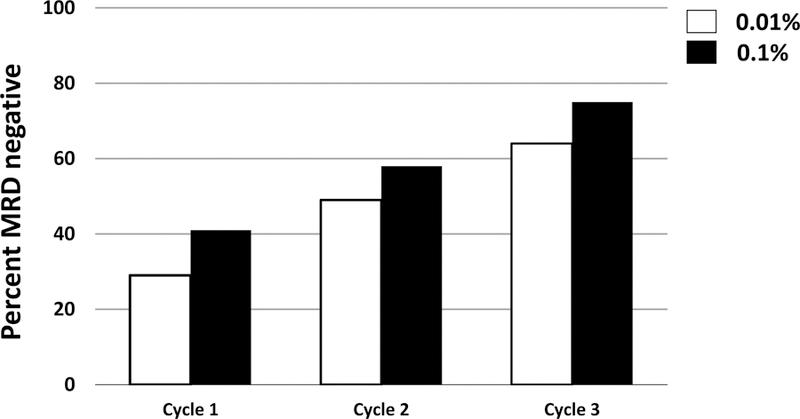
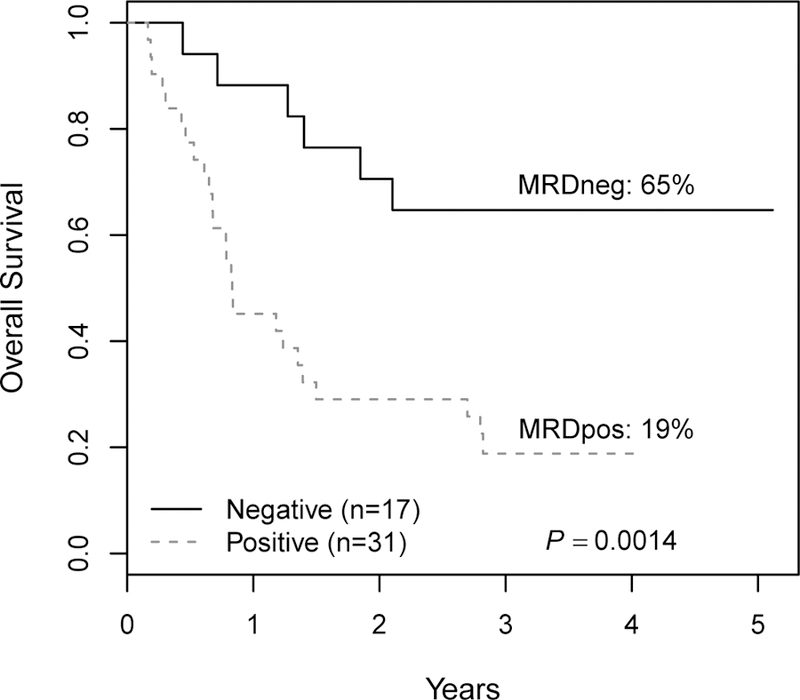
While survival in paediatric acute lymphoblastic leukaemia (ALL) is excellent, survival following relapse is poor. Previous studies suggest proteasome inhibition with chemotherapy improves relapse ALL response rates. This phase 2 Children's Oncology Group study tested the hypothesis that adding the proteasome inhibitor bortezomib to chemotherapy increases complete response rates (CR2). Evaluable patients (n = 135, 103 B-ALL, 22 T-ALL, 10 T-lymphoblastic lymphoma) were treated with reinduction chemotherapy plus bortezomib. Overall CR2 rates were 68 ± 5% for precursor B-ALL patients (<21 years of age), 63 ± 7% for very early relapse (<18 months from diagnosis) and 72 ± 6% for early relapse (18-36 months from diagnosis). Relapsed T-ALL patients had an encouraging CR2 rate of 68 ± 10%. End of induction minimal residual disease (MRD) significantly predicted survival. MRD negative (MRDneg; MRD <0·01%) rates increased from 29% (post-cycle 1) to 64% following cycle 3. Very early relapse, end-of-induction MRDneg precursor B-ALL patients had 70 ± 14% 3-year event-free (EFS) and overall survival (OS) rates, vs. 3-year EFS/OS of 0-3% (P = 0·0001) for MRDpos (MRD ≥0·01) patients. Early relapse patients had similar outcomes (MRDneg 3-year EFS/OS 58-65% vs. MRDpos 10-19%, EFS P = 0·0014). These data suggest that adding bortezomib to chemotherapy in certain ALL subgroups, such as T-cell ALL, is worthy of further investigation. This study is registered at http://www.clinical.trials.gov as NCT00873093.
Keywords: acute lymphoblastic leukaemia; acute lymphocytic leukaemia; minimal residual disease; paediatric leukaemia; proteasome inhibition.
© 2019 British Society for Haematology and John Wiley & Sons Ltd.
Figures





References
-
- Berg SL, Blaney SM, Devidas M, Lampkin TA, Murgo A, Bernstein M, Billett A, Kurtzberg J, Reaman G, Gaynon P, Whitlock J, Krailo M, & Harris MB (2005) Phase II study of nelarabine (compound 506U78) in children and young adults with refractory T-cell malignancies: a report from the Children’s Oncology Group. J.Clin.Oncol, 23, 3376–3382. - PubMed
-
- Bertaina A, Vinti L, Strocchio L, Gaspari S, Caruso R, Algeri M, Coletti V, Gurnari C, Romano M, Cefalo MG, Girardi K, Trevisan V, Bertaina V, Merli P, & Locatelli F (2017) The combination of bortezomib with chemotherapy to treat relapsed/refractory acute lymphoblastic leukaemia of childhood. Br.J.Haematol, 176, 629–636. - PubMed
-
- Bhadri VA, Trahair TN, & Lock RB (2012) Glucocorticoid resistance in paediatric acute lymphoblastic leukaemia. J.Paediatr.Child.Health, 48, 634–640. - PubMed
-
- Borowitz MJ, Devidas M, Hunger SP, Bowman WP, Carroll AJ, Carroll WL, Linda S, Martin PL, Pullen DJ, Viswanatha D, Willman CL, Winick N, & Camitta BM (2008) Clinical significance of minimal residual disease in childhood acute lymphoblastic leukemia and its relationship to other prognostic factors: a Children’s Oncology Group study. Blood, 111, 5477–5485. - PMC - PubMed
-
- Borowitz MJ, Wood BL, Devidas M, Loh ML, Raetz EA, Salzer WL, Nachman JB, Carroll AJ, Heerema NA, Gastier-Foster JM, Willman CL, Dai Y, Winick NJ, Hunger SP, Carroll WL, & Larsen E (2015) Prognostic significance of minimal residual disease in high risk B-ALL: a report from Children’s Oncology Group study AALL0232. Blood, 126, 964–971. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
