

Prevalence of Unexplained Left Ventricular Hypertrophy by Cardiac Magnetic Resonance Imaging in MESA
- PMID: 30957681
- PMCID: PMC6507185
- DOI: 10.1161/JAHA.119.012250
Prevalence of Unexplained Left Ventricular Hypertrophy by Cardiac Magnetic Resonance Imaging in MESA
Abstract
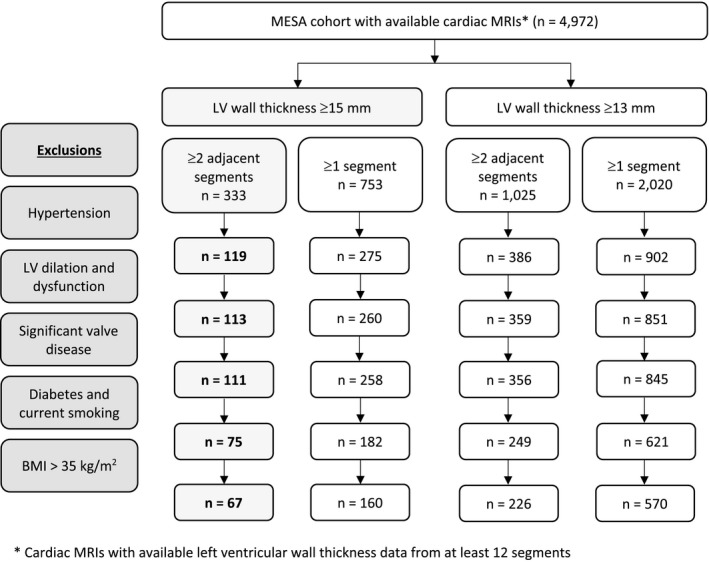
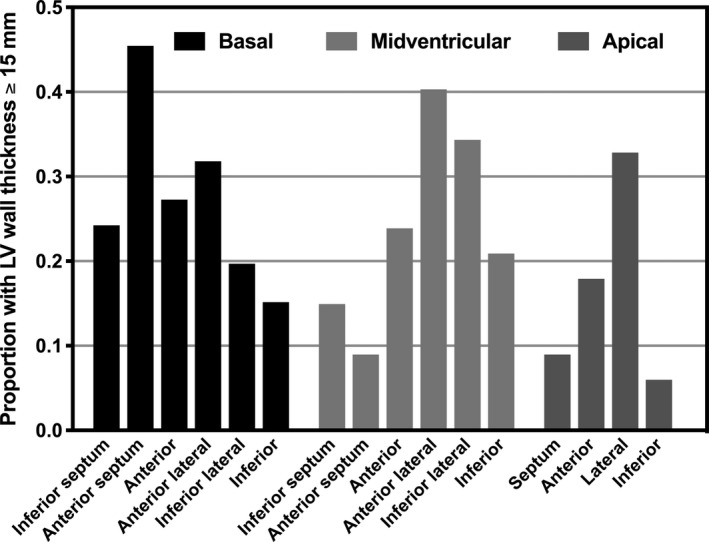
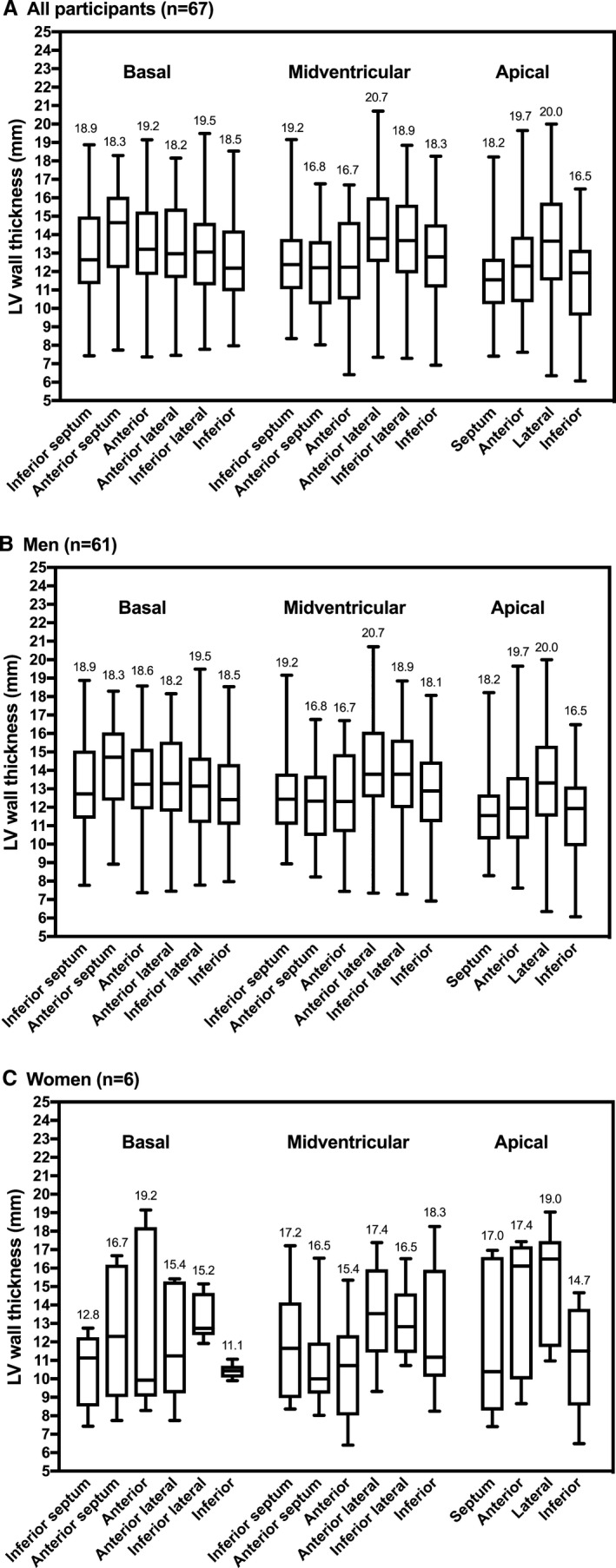
Background Hypertrophic cardiomyopathy is defined as unexplained left ventricular ( LV ) hypertrophy (wall thickness ≥15 mm) and is prevalent in 0.2% of adults (1:500) in population-based studies using echocardiography. Cardiac magnetic resonance imaging ( MRI ) allows for more accurate wall thickness measurement across the entire ventricle than echocardiography. The prevalence of unexplained LV hypertrophy by cardiac MRI is unknown. MESA (Multi-Ethnic Study of Atherosclerosis) recruited individuals without overt cardiovascular disease 45 to 84 years of age. Methods and Results We studied 4972 individuals who underwent measurement of regional LV wall thickness by cardiac MRI as part of the MESA baseline exam. American Heart Association criteria were used to define LV segments. We excluded participants with hypertension, LV dilation (≥95% predicted end-diastolic volume) or dysfunction (ejection fraction ≤50%), moderate-to-severe left-sided valve lesions by cardiac MRI , severe aortic valve calcification by cardiac computed tomography (aortic valve Agatston calcium score >1200 in women or >2000 in men), obesity (body mass index >35 kg/m2), diabetes mellitus, and current smoking. Sixty-seven participants (aged 64±10 years, 9% female) had unexplained LV hypertrophy (wall thickness ≥15 mm in at least 2 adjacent LV segments), representing 1.4% (1 in 74) participants, 2.6% of men and 0.2% of women. Prevalence was similar across categories of race/ethnicity. Hypertrophy was focal in 17 (25.4%), intermediate in 44 (65.7%), and diffuse in 5 (7.5%) participants. Conclusions The prevalence of unexplained LV hypertrophy in a population-based cohort using cardiac MRI was 1.4%. This may have implications for the diagnosis of patients with hypertrophic cardiomyopathy and will require further study.
Keywords: hypertrophic cardiomyopathy; magnetic resonance imaging; population‐based study.
Figures
References
-
- Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, Naidu SS, Nishimura RA, Ommen SR, Rakowski H, Seidman CE, Towbin JA, Udelson JE, Yancy CW; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons . 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124:e783–e831. - PubMed
-
- Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, Charron P, Hagege AA, Lafont A, Limongelli G, Mahrholdt H, McKenna WJ, Mogensen J, Nihoyannopoulos P, Nistri S, Pieper PG, Pieske B, Rapezzi C, Rutten FH, Tillmanns C, Watkins H. 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy: the task force for the diagnosis and management of hypertrophic cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014;35:2733–2779. - PubMed
-
- Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA Study. Coronary Artery Risk Development in (YOUNG) Adults. Circulation. 1995;92:785–789. - PubMed
-
- Maro EE, Janabi M, Kaushik R. Clinical and echocardiographic study of hypertrophic cardiomyopathy in Tanzania. Trop Doct. 2006;36:225–227. - PubMed
-
- Codd MB, Sugrue DD, Gersh BJ, Melton LJ III. Epidemiology of idiopathic dilated and hypertrophic cardiomyopathy. A population‐based study in Olmsted County, Minnesota, 1975–1984. Circulation. 1989;80:564–572. - PubMed
Publication types
MeSH terms
Grants and funding
- N01HC95159/HL/NHLBI NIH HHS/United States
- N01HC95160/HL/NHLBI NIH HHS/United States
- N01HC95161/HL/NHLBI NIH HHS/United States
- N01HC95162/HL/NHLBI NIH HHS/United States
- N01HC95163/HL/NHLBI NIH HHS/United States
- N01HC95164/HL/NHLBI NIH HHS/United States
- N01HC95165/HL/NHLBI NIH HHS/United States
- N01HC95166/HL/NHLBI NIH HHS/United States
- N01HC95167/HL/NHLBI NIH HHS/United States
- N01HC95168/HL/NHLBI NIH HHS/United States
- N01HC95169/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- K24 HL135413/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
