

Nationally-representative serostudy of dengue in Bangladesh allows generalizable disease burden estimates
- PMID: 30958263
- PMCID: PMC6513551
- DOI: 10.7554/eLife.42869
Nationally-representative serostudy of dengue in Bangladesh allows generalizable disease burden estimates
Abstract
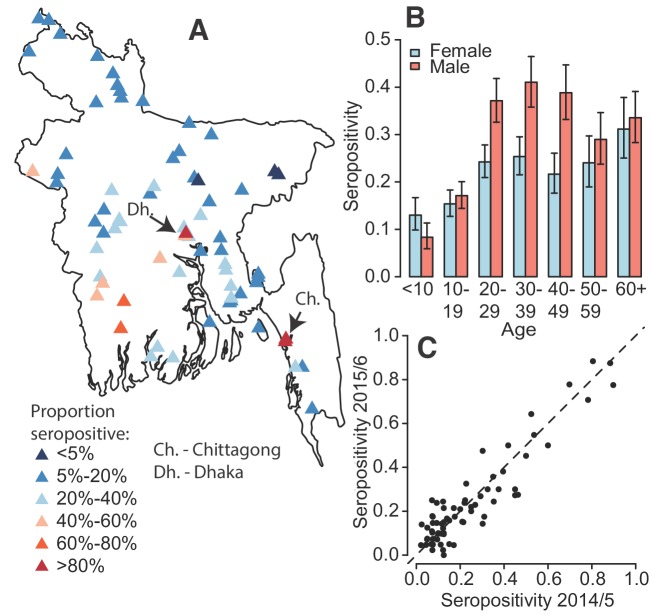
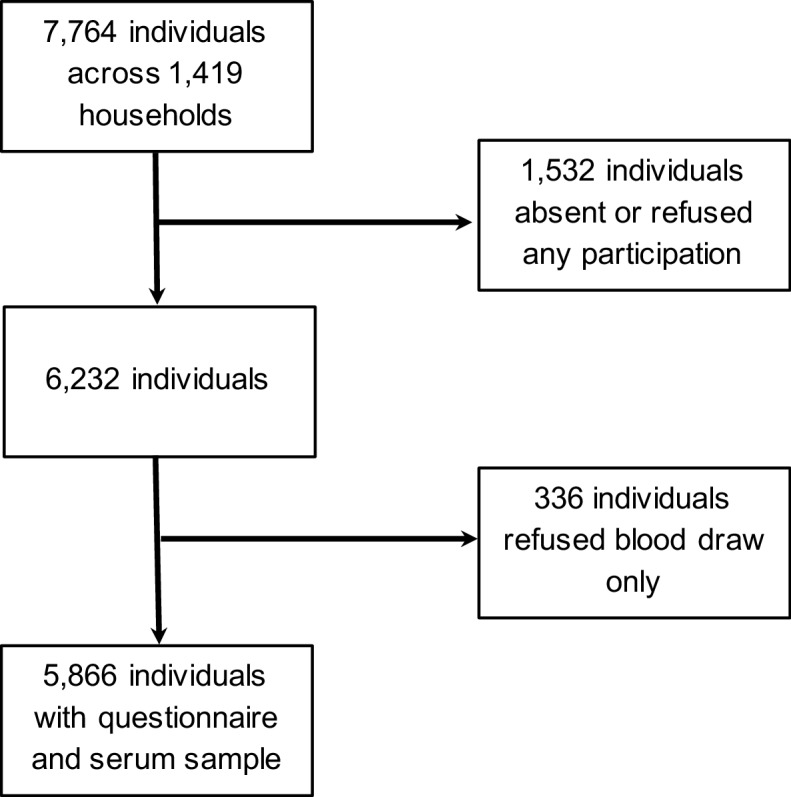
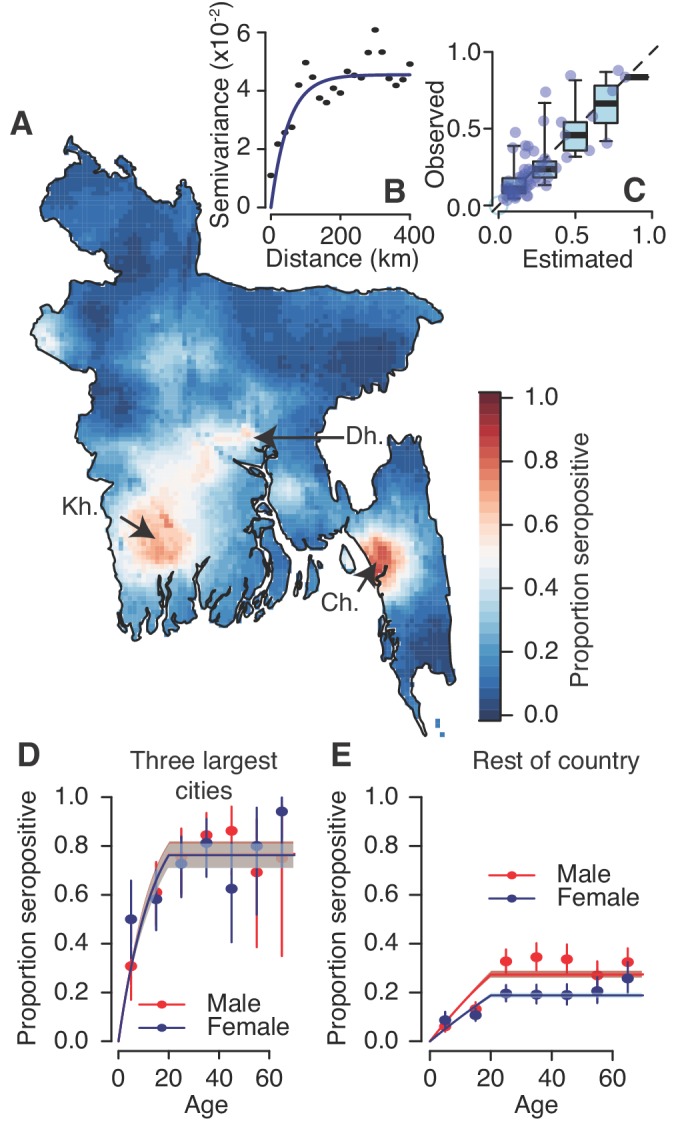
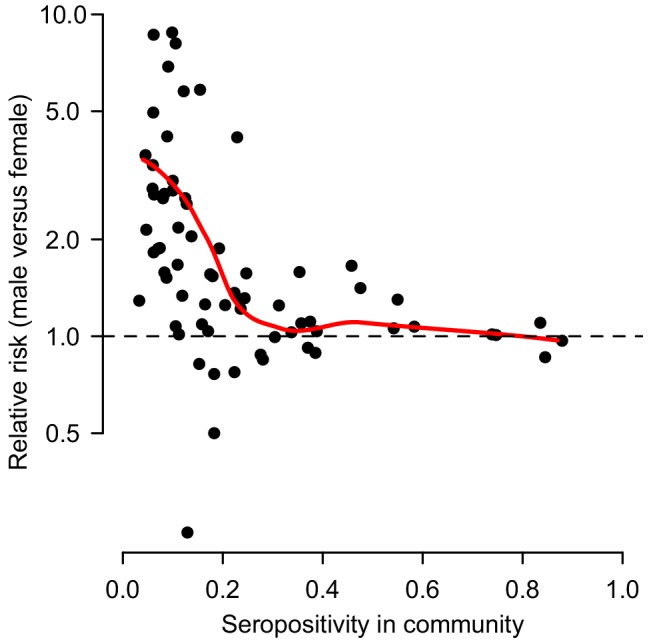
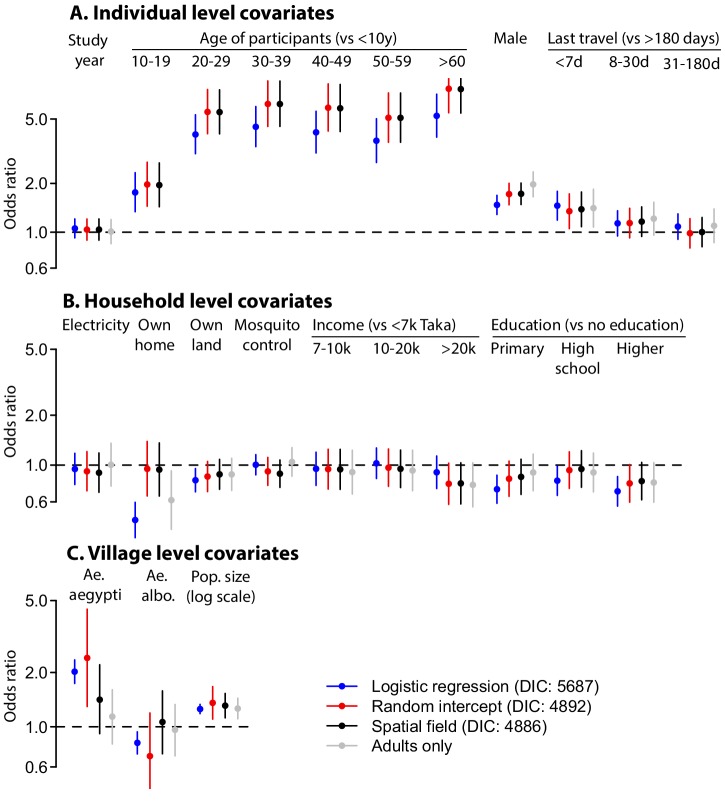
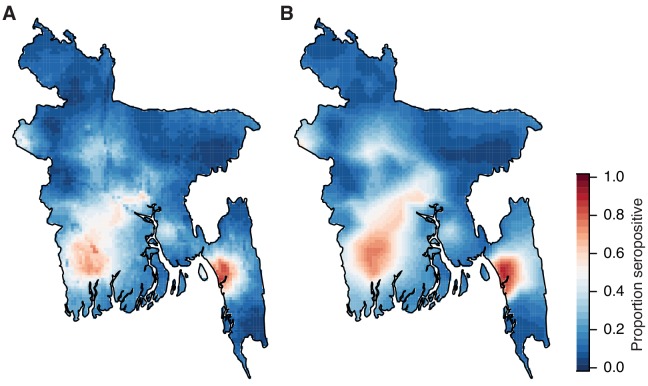
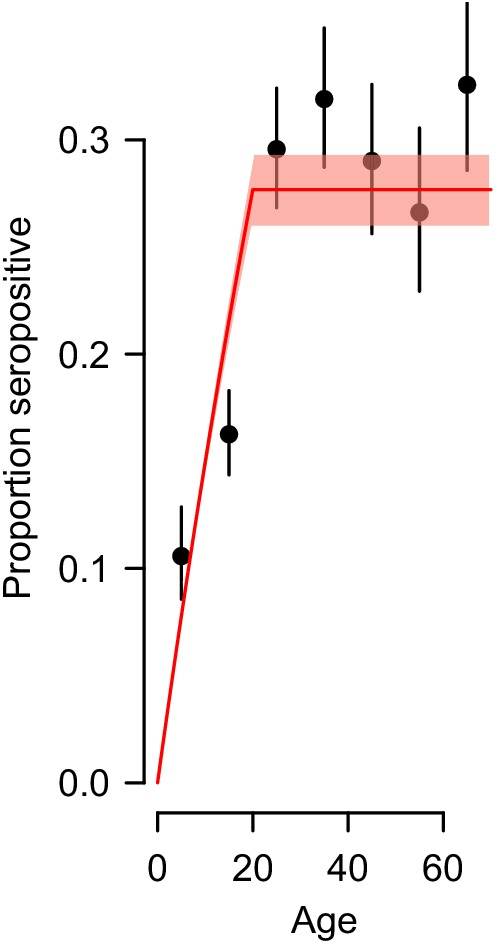
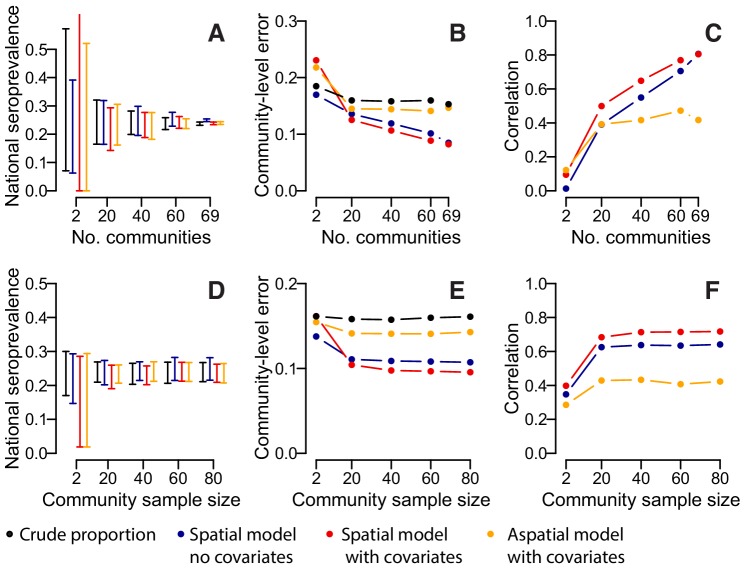
Serostudies are needed to answer generalizable questions on disease risk. However, recruitment is usually biased by age or location. We present a nationally-representative study for dengue from 70 communities in Bangladesh. We collected data on risk factors, trapped mosquitoes and tested serum for IgG. Out of 5866 individuals, 24% had evidence of historic infection, ranging from 3% in the north to >80% in Dhaka. Being male (aOR:1.8, [95%CI:1.5-2.0]) and recent travel (aOR:1.3, [1.1-1.8]) were linked to seropositivity. We estimate that 40 million [34.3-47.2] people have been infected nationally, with 2.4 million ([1.3-4.5]) annual infections. Had we visited only 20 communities, seropositivity estimates would have ranged from 13% to 37%, highlighting the lack of representativeness generated by small numbers of communities. Our findings have implications for both the design of serosurveys and tackling dengue in Bangladesh.
Keywords: Bangladesh; Seroprevalence; dengue; epidemiology; global health; nationally-representative; virus.
Conflict of interest statement
HS, KP, RP, IR, ZR, MA, MR, HA, JH, EG No competing interests declared
Figures
Comment in
- doi: 10.7554/eLife.47458
References
-
- Bhatt S, Gething PW, Brady OJ, Messina JP, Farlow AW, Moyes CL, Drake JM, Brownstein JS, Hoen AG, Sankoh O, Myers MF, George DB, Jaenisch T, Wint GR, Simmons CP, Scott TW, Farrar JJ, Hay SI. The global distribution and burden of dengue. Nature. 2013;496:504–507. doi: 10.1038/nature12060. - DOI - PMC - PubMed
-
- Braks MAH, Honório NA, Lounibos LP, Lourenço-De-Oliveira R, Juliano SA. Interspecific competition between two invasive species of container mosquitoes, Aedes aegypti andAedes albopictus (Diptera: Culicidae), in Brazil. Annals of the Entomological Society of America. 2004;97:130–139. doi: 10.1603/0013-8746(2004)097[0130:ICBTIS]2.0.CO;2. - DOI
-
- Ferguson NM, Donnelly CA, Anderson RM. Transmission dynamics and epidemiology of dengue: insights from age-stratified sero-prevalence surveys. Philosophical Transactions of the Royal Society of London. Series B: Biological Sciences. 1999;354:757–768. doi: 10.1098/rstb.1999.0428. - DOI - PMC - PubMed
