

Endovascular Thrombectomy as a Means to Improve Survival in Acute Ischemic Stroke: A Meta-analysis
- PMID: 30958530
- PMCID: PMC6583698
- DOI: 10.1001/jamaneurol.2019.0525
Endovascular Thrombectomy as a Means to Improve Survival in Acute Ischemic Stroke: A Meta-analysis
Abstract
Importance: Although endovascular thrombectomy (EVT) in acute ischemic stroke is recommended by guidelines to improve functional recovery, thus far there are insufficient data on its association with mortality.
Objective: To identify guideline-relevant trials of EVT vs medical therapy reporting 90-day mortality and perform a meta-analysis.
Data sources: All randomized clinical trials cited for recommendations on EVT vs medical therapy in the latest 2018 American Stroke Association/American Heart Association guidelines.
Study selection: Ten American Stroke Association/American Heart Association guideline-relevant randomized clinical trials of EVT vs medical therapy were selected for inclusion. Two EVT trials were excluded owing to infrequent use of EVT.
Data extraction and synthesis: Data were abstracted by 2 independent investigators and double-checked by 4 others. Singular study data were integrated using the Cochran-Mantel-Haenszel method and a random-effects model to compute summary statistics of risk ratios (RR) with 95% CIs.
Main outcomes and measures: Risk of 90-day mortality and 90-day intracranial hemorrhage was analyzed; sensitivity analyses were performed in early-window EVT trials (which included patients from the onset of symptoms onward) vs late-window EVT trials (which included patients from 6 hours after onset of symptoms onward).
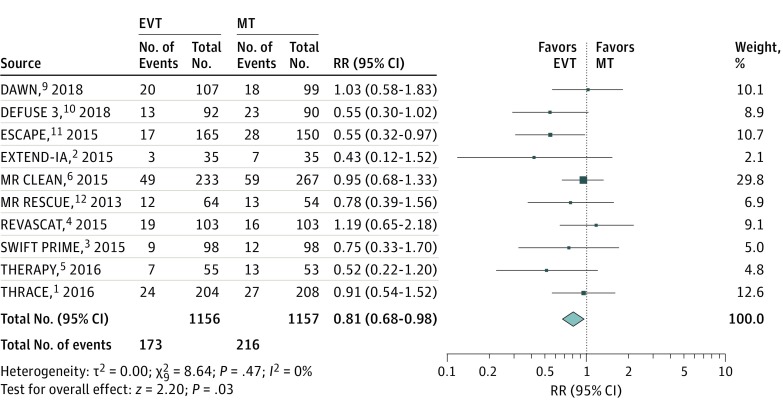
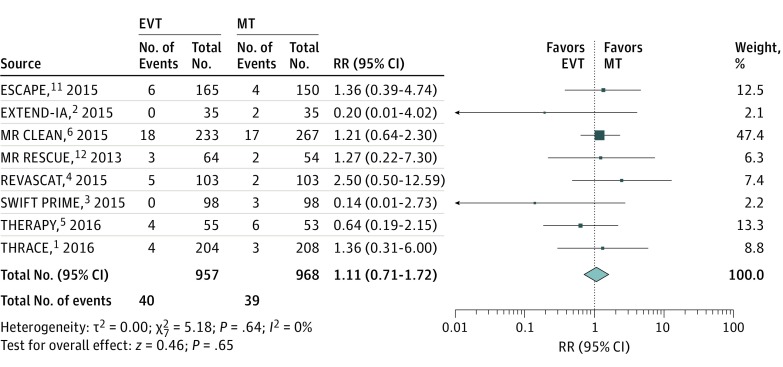
Results: In 10 trials with 2313 patients, EVT significantly reduced the risk for 90-day mortality by 3.7% compared with medical therapy (15.0% vs 18.7%; RR, 0.81; 95% CI, 0.68-0.98; P = .03). Trends were similar in early-window (RR, 0.83; 95% CI, 0.67-1.01; P = .06) and late-window trials only (RR, 0.76; 95% CI, 0.41-1.40; P = .38). There was no difference in the risk for intracranial hemorrhage in EVT vs medical therapy (4.2% vs 4.0%; RR, 1.11; 95% CI, 0.71-1.72; P = .65). Limitations of the studies include trial protocol heterogeneity and bias originating from prematurely terminated trials.
Conclusions and relevance: This meta-analysis of all evidence on EVT cited in the 2018 American Stroke Association/American Heart Association guidelines shows significant benefits for survival during the first 90 days after acute ischemic stroke compared with medical therapy alone.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
