

Stereotactic Body Radiation Therapy for Localized Prostate Cancer: A Systematic Review and Meta-Analysis of Over 6,000 Patients Treated On Prospective Studies
- PMID: 30959121
- PMCID: PMC6770993
- DOI: 10.1016/j.ijrobp.2019.03.051
Stereotactic Body Radiation Therapy for Localized Prostate Cancer: A Systematic Review and Meta-Analysis of Over 6,000 Patients Treated On Prospective Studies
Abstract
Purpose: Utilization of stereotactic body radiation therapy (SBRT) for treatment of localized prostate cancer is increasing. Guidelines and payers variably support the use of prostate SBRT. We therefore sought to systematically analyze biochemical recurrence-free survival (bRFS), physician-reported toxicity, and patient-reported outcomes after prostate SBRT.
Methods and materials: A systematic search leveraging Medline via PubMed and EMBASE for original articles published between January 1990 and January 2018 was performed. This was supplemented by abstracts with sufficient extractable data from January 2013 to March 2018. All prospective series assessing curative-intent prostate SBRT for localized prostate cancer reporting bRFS, physician-reported toxicity, and patient-reported quality of life with a minimum of 1-year follow-up were included. The study was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. Meta-analyses were performed with random-effect modeling. Extent of heterogeneity between studies was determined by the I2 and Cochran's Q tests. Meta-regression was performed using Hartung-Knapp methods.
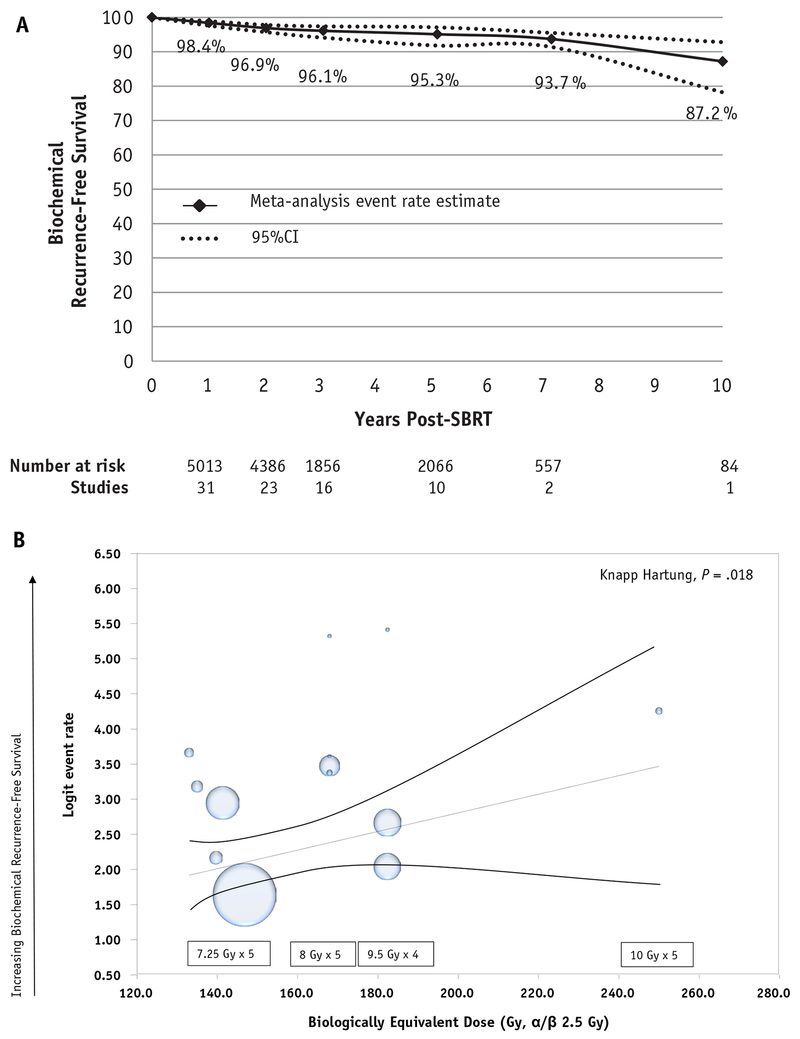
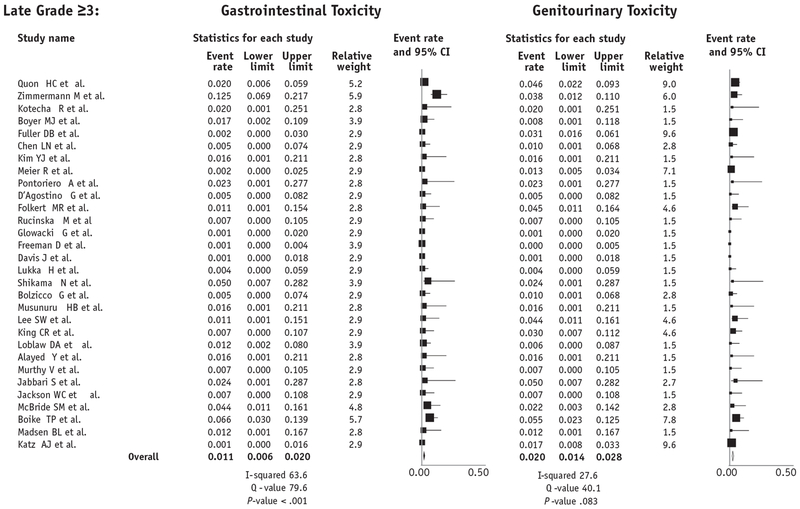
Results: Thirty-eight unique prospective series were identified comprising 6116 patients. Median follow-up was 39 months across all patients (range, 12-115 months). Ninety-two percent, 78%, and 38% of studies included low, intermediate, and high-risk patients. Overall, 5- and 7-year bRFS rates were 95.3% (95% confidence interval [CI], 91.3%-97.5%) and 93.7% (95% CI, 91.4%-95.5%), respectively. Estimated late grade ≥3 genitourinary and gastrointestinal toxicity rates were 2.0% (95% CI, 1.4%-2.8%) and 1.1% (95% CI, 0.6%-2.0%), respectively. By 2 years post-SBRT, Expanded Prostate Cancer Index Composite urinary and bowel domain scores returned to baseline. Increasing dose of SBRT was associated with improved biochemical control (P = .018) but worse late grade ≥3 GU toxicity (P = .014).
Conclusions: Prostate SBRT has substantial prospective evidence supporting its use, with favorable tumor control, patient-reported quality of life, and levels of toxicity demonstrated. SBRT has sufficient evidence to be supported as a standard treatment option for localized prostate cancer while ongoing trials assess its potential superiority.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures



References
-
- Hodges JC, Lotan Y, Boike TP, Benton R, Barrier A, Timmerman RD. Cost-effectiveness analysis of stereotactic body radiation therapy versus intensity-modulated radiation therapy: An emerging initial radiation treatment option for organ-confined prostate cancer. J Oncol Pract 2012;8:e31s–e37s. - PMC - PubMed
