

Predicting the future of ALS: the impact of demographic change and potential new treatments on the prevalence of ALS in the United Kingdom, 2020-2116
- PMID: 30961394
- PMCID: PMC6567553
- DOI: 10.1080/21678421.2019.1587629
Predicting the future of ALS: the impact of demographic change and potential new treatments on the prevalence of ALS in the United Kingdom, 2020-2116
Abstract
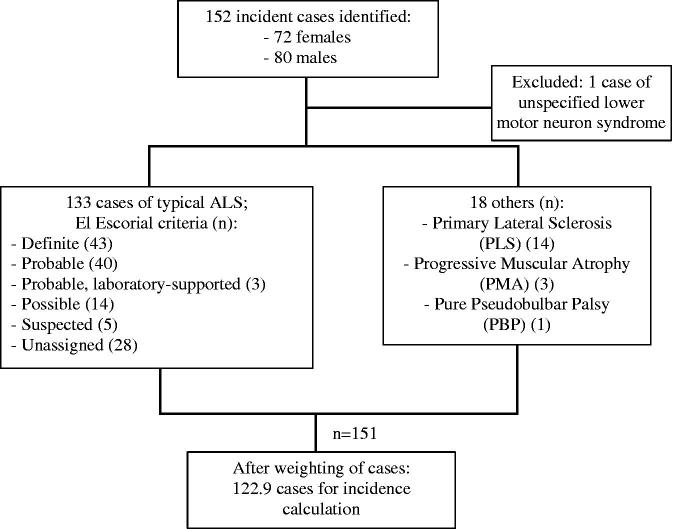
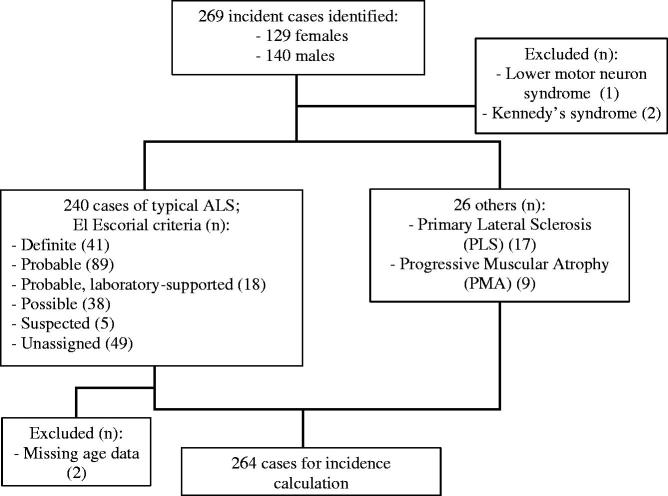
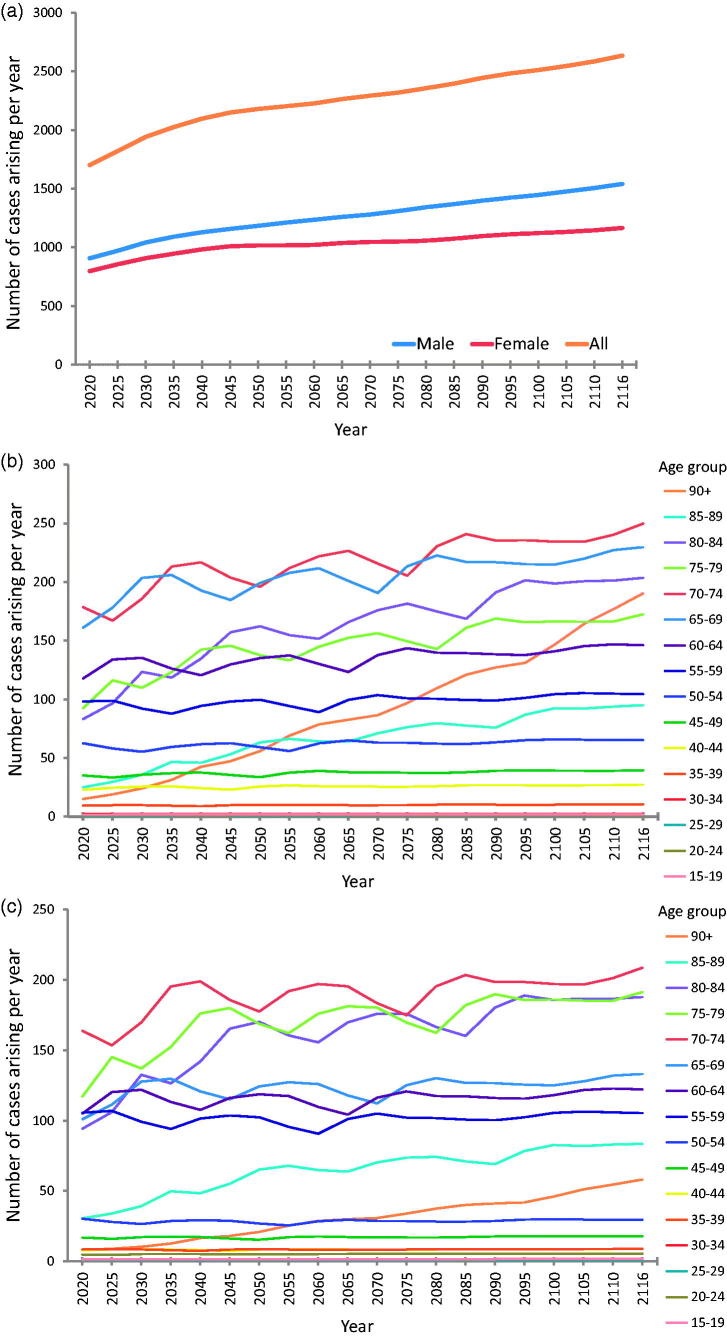
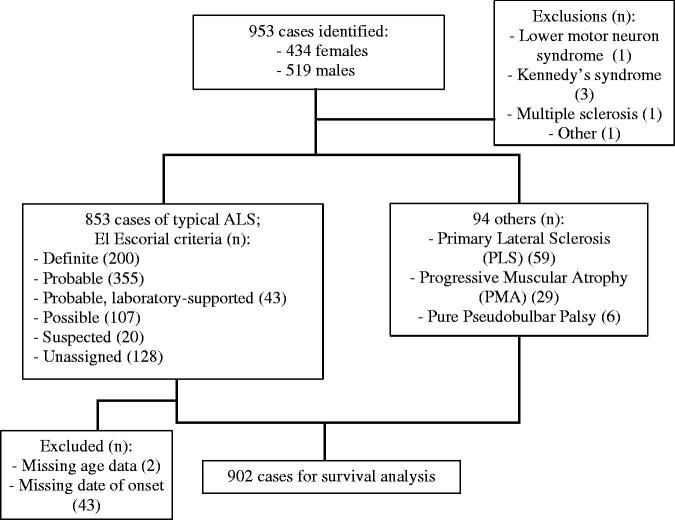
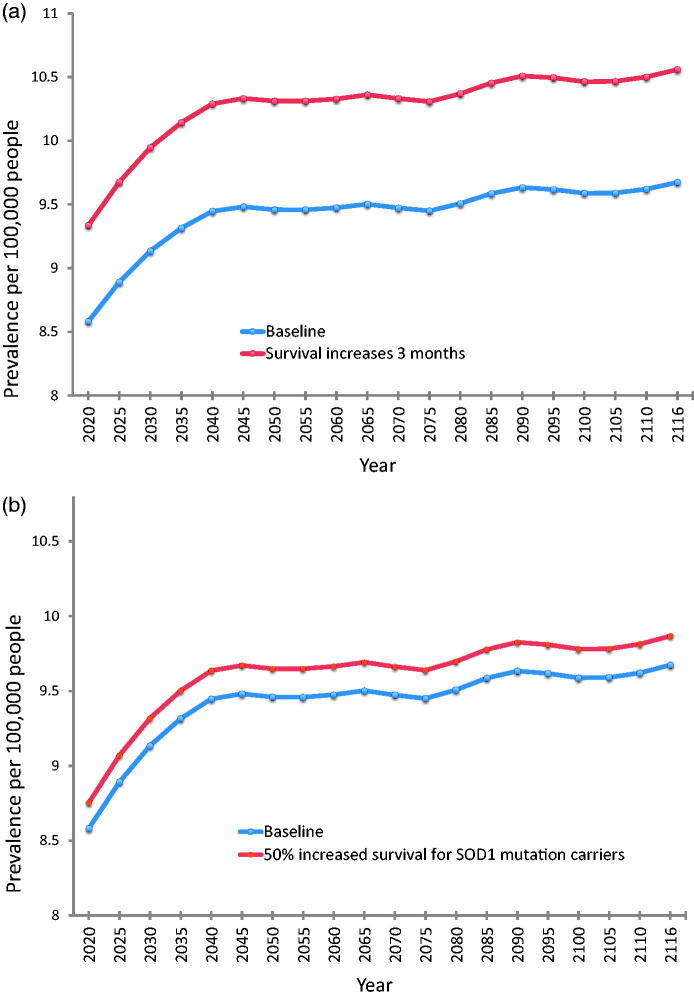
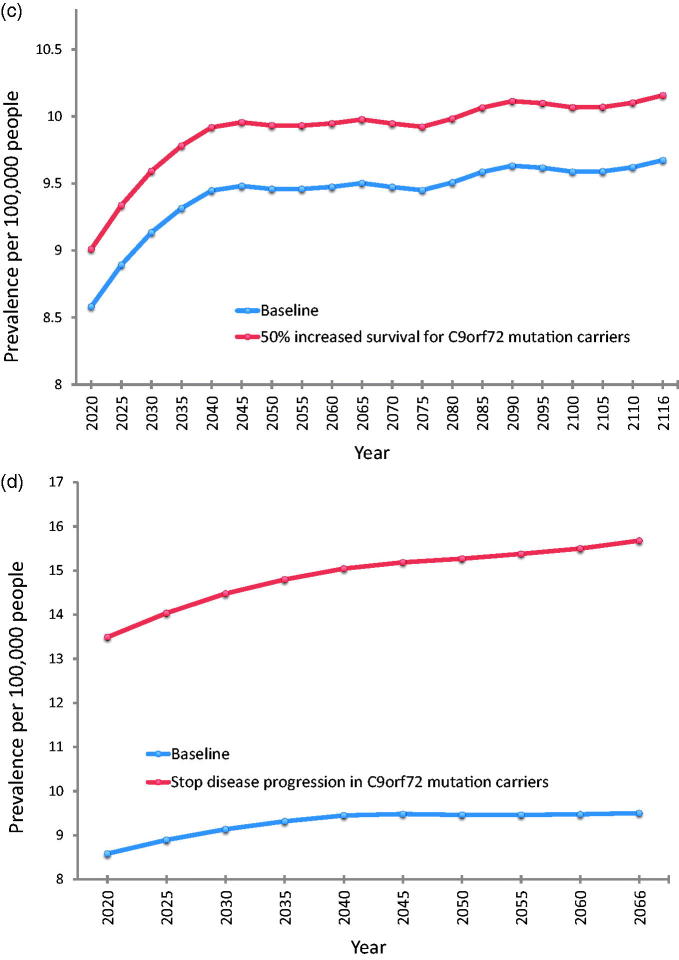
Objective: To model the effects of demographic change under various scenarios of possible future treatment developments in ALS. Methods: Patients diagnosed with ALS at the King's College Hospital Motor Nerve Clinic between 2004 and 2017, and living within the London boroughs of Lambeth, Southwark, and Lewisham (LSL), were included as incident cases. We also ascertained incident cases from the Canterbury region over the same period. Future incidence of ALS was estimated by applying the calculated age- and sex-specific incidence rates to the UK population projections from 2020 to 2116. The number of prevalent cases for each future year was estimated based on an established method. Assuming constant incidence, we modelled four possible future prevalence scenarios by altering the median disease duration for varying subsets of the population, to represent the impact of new treatments. Results: The total number of people newly diagnosed with ALS per year in the UK is projected to rise from a baseline of 1415 UK cases in 2010 to 1701 in 2020 and 2635 in 2116. Overall prevalence of ALS was predicted to increase from 8.58 per 100,000 persons in 2020 to 9.67 per 100,000 persons in 2116. Halting disease progression in patients with C9orf72 mutations would yield the greatest impact of the modelled treatment scenarios, increasing prevalence in the year 2066 from a baseline of 9.50 per 100,000 persons to 15.68 per 100,000 persons. Conclusions: Future developments in treatment would combine with the effects of demographic change to result in more people living longer with ALS.
Keywords: Epidemiology; genetics; models; survival; therapy.
Figures
References
-
- McGuire V, Longstreth WT Jr., Koepsell TD, van Belle G. Incidence of amyotrophic lateral sclerosis in three counties in western Washington state. Neurology. 1996;47:571–3. - PubMed
-
- Mulder DW, Kurland LT. Motor neuron disease: epidemiologic studies. Adv Exp Med Biol. 1987;209:325–32. - PubMed
-
- Johnston CA, Stanton BR, Turner MR, Gray R, Blunt AH, Butt D, et al. . Amyotrophic lateral sclerosis in an urban setting: a population based study of inner city London. J Neurol. 2006;253:1642–3. - PubMed
-
- United Nations, Department of Economic and Social Affairs, Population Division. 2013. World Population Ageing 2013. ST/ESA/SER.A/348.http://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldP...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous