

Bowel obstruction caused by colonic metastasis of lung adenocarcinoma: a case report and literature review
- PMID: 30961608
- PMCID: PMC6454752
- DOI: 10.1186/s12957-019-1611-y
Bowel obstruction caused by colonic metastasis of lung adenocarcinoma: a case report and literature review
Abstract
Introduction: Lung cancer is the most common cause of cancer-related deaths globally. Metastatic disease is often found at the time of initial diagnosis in the majority of lung cancer patients. However, colonic metastases are rare. This report describes an uncommon case of colonic metastasis from lung adenocarcinoma.
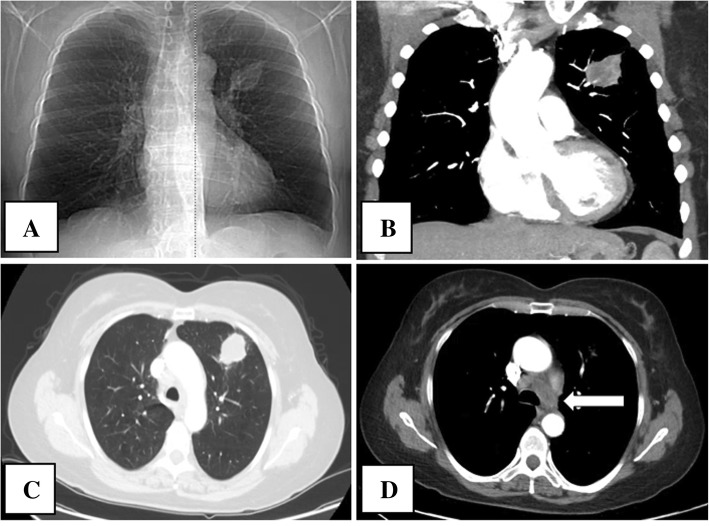
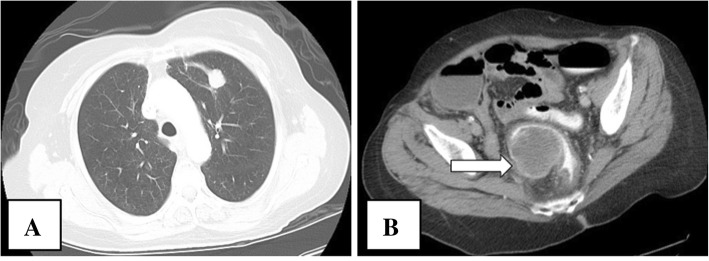
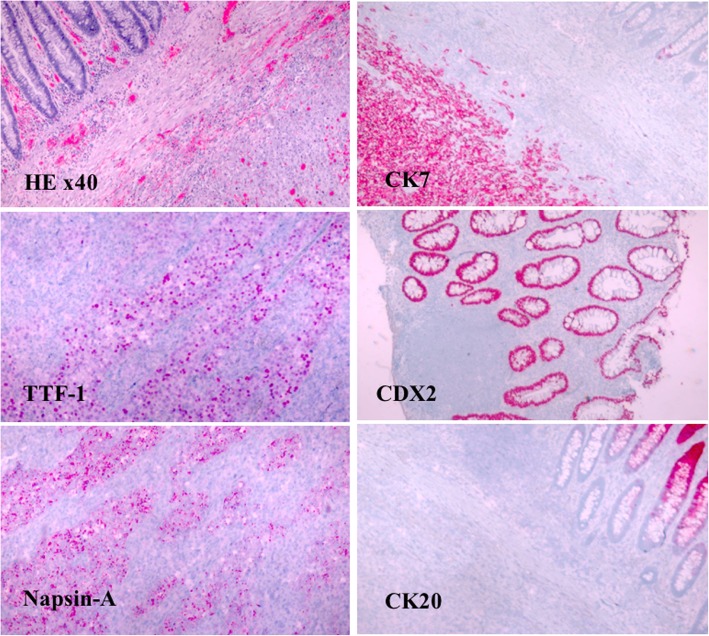
Case presentation: A 64-year-old female presented to her gastroenterologist for progressively worsening abdominal pain and constipation. Exploratory colonoscopy revealed a large rectosigmoid mass resulting in near total rectal occlusion. Her specialist recommended she immediately go to her regional hospital for further workup. On admission, she complained of continued abdominal pain and constipation. Notably, she had a past medical history of non-small cell lung cancer (T1bN3M0 stage IIIB), diagnosed 1 year prior. She was thought to be in remission following radiation and immunotherapy with pembrolizumab. Upon hospital admission, she underwent an urgent colostomy, ileocecectomy and anastomosis, and rectosigmoid mass resection with tissue sampling. Pathology confirmed the diagnosis of colonic metastasis from primary lung adenocarcinoma. Treatment was with systemic chemotherapy followed by localized radiation to the pelvic region was started. She did not respond well to these therapies. Subsequent imaging showed refractory tumor growth in the pelvic region. Treatment could not be completed due to the patient experiencing a debilitating stroke, and she was transitioned to hospice care.
Conclusions: Clinicians should have a low threshold for intestinal investigation and considerations for colonic metastasis when patients with a history of primary lung cancer have abdominal symptoms.
Keywords: Colonic metastasis; Non-small cell lung cancer; Primary lung cancer.
Conflict of interest statement
Ethics approval and consent to participate
The data collection on the patient had been approved by the local Ethical Committee.
Consent for publication
Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient/parent/guardian/ relative of the patient.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Colonic Metastasis of Lung Adenocarcinoma: A Case Report.Cureus. 2019 Mar 28;11(3):e4341. doi: 10.7759/cureus.4341. Cureus. 2019. PMID: 31187006 Free PMC article.
-
Usefulness of a Colonic Stent for Colonic Obstruction Caused by Lung Cancer Metastasis.J Nippon Med Sch. 2021 Dec 29;88(6):556-560. doi: 10.1272/jnms.JNMS.2021_88-514. Epub 2020 Nov 30. J Nippon Med Sch. 2021. PMID: 33250481
-
Solitary colonic metastasis from primary lung adenocarcinoma first presenting as intestinal obstruction: A case report.Medicine (Baltimore). 2019 Jan;98(3):e14063. doi: 10.1097/MD.0000000000014063. Medicine (Baltimore). 2019. PMID: 30653118 Free PMC article.
-
Undiagnosed primary lung carcinoma with initial manifestation of intestinal obstruction: A case report and literature review.J Cancer Res Ther. 2015 Aug;11 Suppl 1:C134-7. doi: 10.4103/0973-1482.163873. J Cancer Res Ther. 2015. PMID: 26323914 Review.
-
[Perforation of the small intestine caused by metastasis from primary lung cancer: report of two cases and the discussion of 48 cases published in the Japanese literature].Nihon Kokyuki Gakkai Zasshi. 2007 May;45(5):430-5. Nihon Kokyuki Gakkai Zasshi. 2007. PMID: 17554989 Review. Japanese.
Cited by
-
Colorectal Metastasis From Lung Adenocarcinoma With Initial Gastrointestinal Symptoms: A Case Report and Literature Review.Thorac Cancer. 2025 Jan;16(2):e15531. doi: 10.1111/1759-7714.15531. Thorac Cancer. 2025. PMID: 39828510 Free PMC article. Review.
-
Case Report: Recurrent colonic metastasis from lung cancer-diagnostic pitfalls and therapeutic challenge of a peculiar case.Front Surg. 2023 Dec 22;10:1288940. doi: 10.3389/fsurg.2023.1288940. eCollection 2023. Front Surg. 2023. PMID: 38186393 Free PMC article.
-
SMARCA4-deficient non-small cell lung cancer with metastasis to the sigmoid colon: a case report.World J Surg Oncol. 2025 Mar 29;23(1):106. doi: 10.1186/s12957-025-03757-7. World J Surg Oncol. 2025. PMID: 40158181 Free PMC article.
-
Successful resection of colonic metastasis of lung cancer after colonic stent placement: A case report and review of the literature.World J Gastrointest Surg. 2023 Jul 27;15(7):1549-1558. doi: 10.4240/wjgs.v15.i7.1549. World J Gastrointest Surg. 2023. PMID: 37555118 Free PMC article.
-
Colon metastasis from lung adenocarcinoma with BRAF V600E mutation: A case report.Front Immunol. 2022 Aug 8;13:970879. doi: 10.3389/fimmu.2022.970879. eCollection 2022. Front Immunol. 2022. PMID: 36003386 Free PMC article.
References
-
- Goldstraw P, Crowley J, Chansky K, Giroux D, Groome P, Rami-Porta R, Postmus P, Rusch V, Sobin L. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2(8):706–714. doi: 10.1097/JTO.0b013e31812f3c1a. - DOI - PubMed
-
- Hori M, Matsuda T, Shibata A, Katanoda K, Sobue T, Nishimoto H. Cancer incidence and incidence rates in Japan in 2009: a study of 32 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn J Clin Oncol. 2015;45(9):884–891. doi: 10.1093/jjco/hyv088. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
