

Association between Policy Changes for Oxygen Saturation Alarm Settings and Neonatal Morbidity and Mortality in Infants Born Very Preterm
- PMID: 30961990
- PMCID: PMC6535348
- DOI: 10.1016/j.jpeds.2019.01.048
Association between Policy Changes for Oxygen Saturation Alarm Settings and Neonatal Morbidity and Mortality in Infants Born Very Preterm
Abstract
Objective: To determine the impact of policy changes for pulse oximetry oxygen saturation (SpO2) alarm limits on neonatal mortality and morbidity among infants born very preterm.
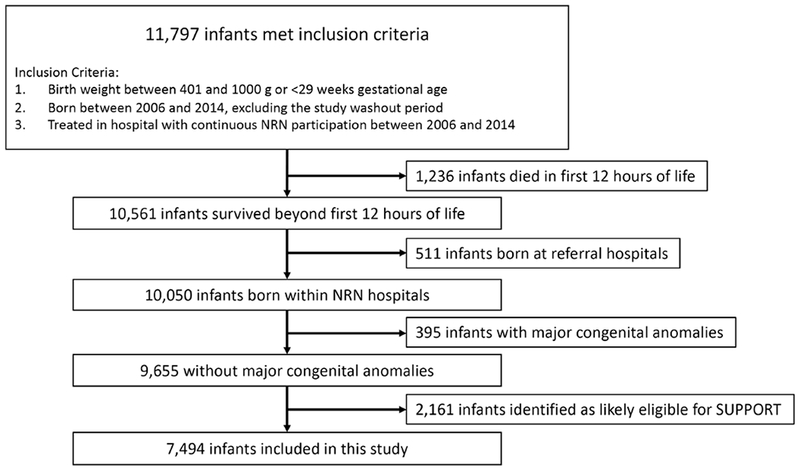
Study design: This was a retrospective cohort study of infants born very preterm in the Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Infants were classified based on treatment at a hospital with an SpO2 alarm policy change and study epoch (before vs after policy change). We used a generalized linear mixed model to determine the effect of hospital group and epoch on the primary outcomes of mortality and severe retinopathy of prematurity (ROP) and secondary outcomes of necrotizing enterocolitis, bronchopulmonary dysplasia, and any ROP.
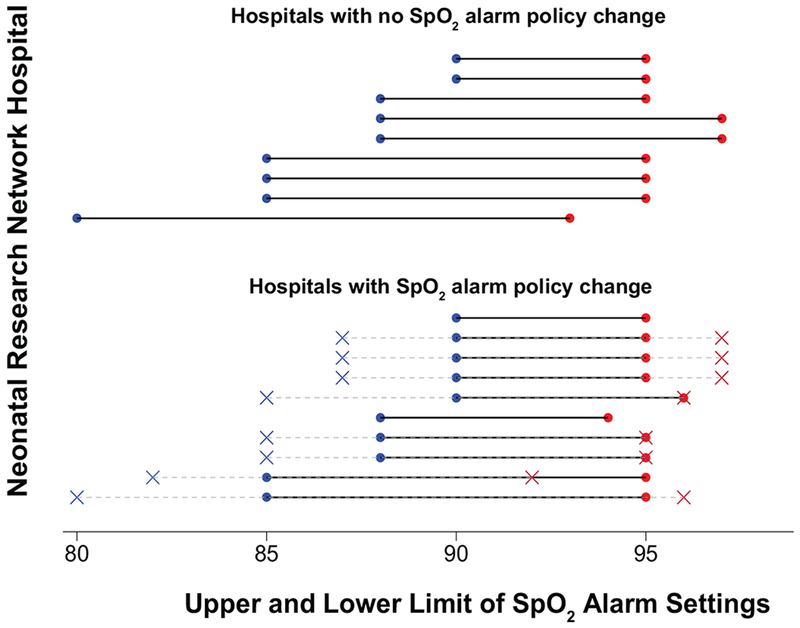
Results: There were 3809 infants in 10 hospitals with an SpO2 alarm policy change and 3685 infants in 9 hospitals without a policy change. The nature of most policy changes was to narrow the SpO2 alarm settings. Mortality was lower in hospitals without a policy change (aOR 0.63; 95% CI 0.50-0.80) but did not differ between epochs in policy change hospitals. The odds of bronchopulmonary dysplasia were greater for hospitals with a policy change (aOR 1.65; 95% CI 1.36-2.00) but did not differ for hospitals without a policy change. Severe ROP and necrotizing enterocolitis did not differ between epochs for either group. The adjusted odds of any ROP were lower in recent years in both hospital groups.
Conclusions: Changing SpO2 alarm policies was not associated with reduced mortality or increased severe ROP among infants born very preterm.
Keywords: mortality; oxygen saturation; preterm; retinopathy of prematurity.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Reply.J Pediatr. 2021 Feb;229:311. doi: 10.1016/j.jpeds.2020.11.006. Epub 2020 Nov 9. J Pediatr. 2021. PMID: 33181196 No abstract available.
-
Clarification of aOR calculation.J Pediatr. 2021 Feb;229:310-311. doi: 10.1016/j.jpeds.2020.11.005. Epub 2020 Nov 9. J Pediatr. 2021. PMID: 33181198 No abstract available.
References
-
- Stenson BJ, Tarnow-Mordi WO, Darlow BA, Simes J, Juszczak E, Askie L, et al. Oxygen saturation and outcomes in preterm infants. N Engl J Med. 2013;368:2094–104. - PubMed
-
- Schmidt B, Whyte RK, Asztalos EV, Moddemann D, Poets C, Rabi Y, et al. Effects of Targeting Higher vs Lower Arterial Oxygen Saturations on Death or Disability in Extremely Preterm Infants: A Randomized Clinical Trial. JAMA. 2013;309:2111–20. - PubMed
Publication types
MeSH terms
Grants and funding
- UL1 TR001111/TR/NCATS NIH HHS/United States
- U10 HD021385/HD/NICHD NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- UG1 HD027904/HD/NICHD NIH HHS/United States
- U10 HD027851/HD/NICHD NIH HHS/United States
- UG1 HD027880/HD/NICHD NIH HHS/United States
- UL1 TR001117/TR/NCATS NIH HHS/United States
- UG1 HD053109/HD/NICHD NIH HHS/United States
- UG1 HD027851/HD/NICHD NIH HHS/United States
- U24 HD095254/HD/NICHD NIH HHS/United States
- U10 HD053089/HD/NICHD NIH HHS/United States
- U10 HD027856/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- UG1 HD027853/HD/NICHD NIH HHS/United States
- U10 HD053109/HD/NICHD NIH HHS/United States
- UG1 HD087229/HD/NICHD NIH HHS/United States
- UG1 HD040689/HD/NICHD NIH HHS/United States
- M01 RR008084/RR/NCRR NIH HHS/United States
- UG1 HD053089/HD/NICHD NIH HHS/United States
- U10 HD040689/HD/NICHD NIH HHS/United States
- U10 HD040492/HD/NICHD NIH HHS/United States
- U10 HD027853/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- K23 HD084727/HD/NICHD NIH HHS/United States
- UG1 HD040492/HD/NICHD NIH HHS/United States
- UG1 HD021364/HD/NICHD NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
